

POSITIVE ID
Making the world’s invisible people, visible
An ID can help improve the lives of the world’s poorest and most vulnerable people.


How do you prove you really are who you say you are? In the U.S. and many rich countries, that’s easy. We have many ways to prove our identity: a birth certificate, a driver’s license, a Social Security card, or a passport.
But imagine for a moment that you are one of the estimated one billion people in the world—most of them among the poorest and the most vulnerable—who have no official identification. No birth certificates. No official ID documents. Nothing.
Without a way to prove who you are, you would face huge problems going to school, seeing a doctor, receiving government services, getting a bank account, finding a job, traveling across a border, or having access to many other rights and services most of us take for granted. Without an ID, you would be nameless in the eyes of the government and largely ignored.
For the last decade, Nandan Nilekani has been working to make these “invisible people,” as he calls them, visible by giving them access to official identification. One of India’s leading technology entrepreneurs, Nandan joined the government of India to lead the launch of India’s national biometric ID system, which uses fingerprints and other biological traits to verify the identities of the country’s more than 1.3 billion residents. This ID system, known as Aadhaar (Hindi for “foundation”), is the world’s largest biometric identification system and has become a valuable platform for delivering social welfare programs and other government services.
Now, Nandan is working with the World Bank Group to help other countries build their own digital identification systems. Advances in biometrics, data management, mobile phones, and other technologies are making it possible to provide people with a verifiable digital identity simply, quickly, and securely. At the same time, there is growing awareness in the global community that with a proof of ID, the world’s poorest people have a powerful tool to be seen, heard, and improve their lives. Giving everyone access to a legal identity is one of the targets of the Global Goals. And more donors, including the Omidyar Network and our foundation, are supporting efforts to achieve this goal.
I first met Nandan more than 20 years ago when he was working to grow Infosys, a technology and consulting corporation he co-founded. I was impressed by him then and continue to be amazed by how he has lent his entrepreneurial passion to philanthropy and public service over the years. (With his wife, Rohini, Nandan also co-founded the EkStep Foundation, which seeks to improve education.)
Nandan’s early thinking about the importance of identification was sketched out in his bestselling book, Imagining India, which explores India’s potential to bridge the gap between rich and poor as it undergoes dramatic economic growth. Verifiable IDs, he predicted in 2008, would be transformational for India’s poorest people. By acknowledging the existence of all its residents with a national ID, he said, the government would be compelled to improve the access and quality of all its services that can uplift the most vulnerable people.
At the time, the government of India was in the process of planning a unique national ID system. In 2009, Nandan was tapped by the government to turn this vision into reality. No one had ever tried to create a digital identification system on this scale before. His team was tasked with gathering fingerprints, iris scans, and a photograph for more than one billion residents of India. Each person who signed up was issued a unique 12-digit identification number that could be used along with their biometric information to prove their identity. This system ensured that someone’s identity could not be faked or duplicated, which had been a common problem in India’s largely paper-based government social welfare programs.
A decade later, Aadhaar has enrolled nearly all residents of India. With a trustworthy system to verify identities of beneficiaries for everything from pensions to food subsidies, the government has been able to save billions of dollars because of reduced fraud and corruption.
Of course, India’s ID system has not been without controversy. There were many privacy concerns, including criticism that the Aadhaar system was a mass surveillance tool and that personal data would be misused. Last year, a landmark decision by the Supreme Court of India found that the program did not violate the privacy rights of the country’s residents. But in order to prevent misuse use of personal data the court placed tight limits on how the ID system could be used and shared.
Nandan stepped down from his government post in 2014. But he continues to lend his voice, both as a writer and speaker, to improve access to digital identification for the world’s poorest people. And as an advisor to the World Bank, Nandan is sharing his experience with Aadhaar to help other countries design and roll out their own digital identification programs.
While progress is being made to launch more identification systems, many people around the world still lack identification of any kind. According to the latest estimates by the World Bank, there are one billion people in the world without an official proof of identity, including 45 percent of the population in sub-Saharan Africa and 17 percent of South Asia’s population.
Thanks to the work Nandan is doing the world is moving closer to the day when everyone will have access to an official ID. The sooner we can achieve this goal, the sooner the world’s poorest residents will not only be able to prove who they are, but also realize their aspirations for better lives.
Life Line
A phone call that saves lives
m-mama uses mobile technology and community drivers to solve one of global health’s most persistent problems: Getting pregnant women to hospitals in time.
In the United States, when someone has a medical emergency, we take for granted that an ambulance will arrive. It will get to some places faster than others—a disparity driven by wealth and other factors. Still, by calling 911, we’re immediately connected to a vast fleet of emergency vehicles plugged into a system that’s designed to get people to hospitals in times of crisis.
But what about countries where ambulances aren’t readily accessible? What about places where even cars are scarce, where the nearest hospital with surgical capacity might be 100 miles away down an unpaved road, and where a family facing a medical crisis has no reliable way to get there or pay for the journey?
This is the reality for millions of pregnant women across sub-Saharan Africa.
Thanks to modern medicine, we now know how to prevent most maternal and newborn deaths. And maternal mortality has declined by 40 percent over the last two decades as a result. But hundreds of thousands of women and babies still die every year from complications during pregnancy and childbirth, because they can’t get to a place where someone can treat them in time.
In maternal health, this problem is called the “second delay.” It’s a terrible tragedy, one that the Gates Foundation has been trying to address for years.
Back in 2013, partners including Vodafone Foundation and local health organizations started tackling this problem by asking a simple question in rural Tanzania: What if you could create something like a 911 system that worked with whatever transportation was available in a community? They tested the idea in a few districts, and it worked well enough that they decided to scale it up. They called it m-mama.
m-mama works like this: When a community healthcare worker identifies an emergency—maybe it’s severe bleeding after delivery, or a premature baby who can’t breathe—they call a free hotline. A trained nurse dispatcher uses an app to figure out what kind of care is needed and where it’s available, then coordinates whatever transportation makes sense for that location (a community driver with a car where there are good roads, a motorcycle where there aren’t, a boat for island communities, even a horse for mountainous terrain.) The dispatcher stays on top of everything, tracking the journey, alerting the receiving facility, and handling payment at the end.
The numbers speak for themselves. Since 2013, m-mama has responded to more than 125,000 emergencies and saved an estimated 5,266 lives. And in regions where m-mama launched, maternal emergency transports more than doubled. That means there was a massive need that was going unmet for far too long. About 58% of the deliveries transported by m-mama end up requiring a C-section, compared to the 10-15% you would expect in the general population. These are genuinely high-risk cases that would have likely ended in tragedy without emergency transport.
What’s especially impressive about m-mama’s impact is that it hasn’t required building new hospitals or buying any expensive equipment. Instead, it makes existing health systems work better by coordinating resources that are already there—ambulances, facilities, healthcare workers—and filling gaps with options that cost a fraction of what traditional ambulances do.
And it is scaling. m-mama started as a pilot serving 750,000 people and now reaches 62 million in Tanzania. It’s gone nationwide in Lesotho. It just launched in Malawi and is scaling up in Kenya. There are plans for more countries across sub-Saharan Africa, supported in part by the Beginnings Fund—a partnership that includes our foundation, the Mohamed bin Zayed Foundation for Humanity, and other organizations working to improve maternal and newborn health across Africa.
The program is financially sustainable too. Once the program is up and running, the governments cover operating costs. m-mama has proven it can be owned and run locally, which is the only way something like this works long-term.
m-mama is a reminder that not all breakthroughs in global health are new drugs or sophisticated technology. Sometimes they’re just smart ways of getting the right care to the right person at the right time. When a mother or baby is in crisis, minutes can make the difference between life and death.
m-mama is making sure those minutes count.
Such great heights
This heroic nurse climbs 1000-foot ladders to save lives
Agnes Nambozo goes to extraordinary lengths to vaccinate children in Uganda.
How do you get to work? Some people roll out of bed and move 10 feet to their desk. Others walk to the office or take public transit. I usually drive a car.
No matter how you get there, I guarantee that your commute isn’t as wild as Agnes Nambozo’s: She regularly climbs a rickety ladder that is nearly 1,000 feet tall—or 300 meters—before she can start work for the day.
Agnes is a nurse based in Buluganya, located in the shadow of Mount Elgon in eastern Uganda. Like many nurses in rural communities across sub-Saharan Africa, she wears a lot of different hats. She might spend one day delivering babies and treating wounds and the next as a health educator, promoting good nutrition and sanitation in her community. The days Agnes believes she makes the biggest difference, though, are the ones when she treks deep into the Ugandan countryside to vaccinate children.
Uganda has done an amazing job of reducing childhood mortality over the last 25 years. In 2000, about 145 children died per every thousand live births. By 2023, that figure had dropped to fewer than 40 deaths per 1,000 births. A lot of that progress can be attributed to vaccines and vaccinators like Agnes.
Eastern Uganda is a gorgeous place, but parts of it are incredibly difficult to cross. Many of the communities Agnes visits are high in the mountains. Some are only accessible by ladders, which act as links between communities. Older children can climb down them to go to school, but they are too steep for the little ones. Mothers can’t safely carry their babies down the ladders to the health clinic, so Agnes comes to them.
When Agnes was a little girl, she wanted to be a police officer—until her mom convinced her the job was too dangerous. Instead, she took a nursing course. She fell in love with the profession, even though it ended up being a much riskier job than her mom ever imagined. She travels to the villages to vaccinate kids in all kinds of weather. It’s often rainy in the mountains, and the ladders become slippery. “The ladders are risky because you might miss a step,” she says. “If you are lucky, you can get a fracture. If you’re not lucky, you can lose your life.”
On the days when she heads into the field to vaccinate children, Agnes leaves her house by 6:00 am. She takes a taxi from where she lives in Sironko to Buyaga, a town closer to where the health clinic is located. Cars can’t drive on the road to the clinic, so she takes a motorbike for the last stretch.
She arrives at the clinic around 8:00 am and starts packing for the day. Rural vaccinators like Agnes must carry their supplies on their backs, and there’s an art to making sure everything is loaded properly. The vaccines must be kept cold so she wears a heavy insulated backpack stuffed with ice packs.
Agnes then hops on another motorbike to a staging location before heading off on foot to the ladders. By the time she reaches the village and starts setting up to immunize the community, it’s usually around 10:30—more than four hours after she left her house for the day.
She comes in with a plan for how many people she’ll vaccinate, but Agnes always brings a couple extra doses just in case. A typical day usually means around 50 patients. Most are children under 5, who get vaccinated against deadly diseases like polio, measles, tetanus, and pneumonia. The latter is especially important in a region as rainy as this one, where the damp weather makes people more susceptible to respiratory diseases.
Agnes and her colleagues are often the only health workers who visit the most remote communities in the mountains, so they also provide general nursing care while they’re there. Agnes regularly gives kids deworming treatments and key supplements like vitamin A. She answers questions from the adults and offers them health guidance, including advice on planning a family.
After she wraps up for the day, Agnes makes the long trek back home. It’s exhausting, difficult work, but she is proud to help so many people. “Our motto for nurses in Uganda is ‘To love and serve,’” she says. “And to me, love is not just a word. It’s a verb.”
Unfortunately, Agnes’s job recently became a lot more difficult. Many of her colleagues at the health clinic in Buluganya were supported by USAID, and they lost their jobs when funding was cut. Some of the positions that were eliminated supported new and expectant mothers. Others worked on HIV and tuberculosis, distributing medication and testing high-risk individuals to prevent further spread.
Agnes and the others who are left are doing their best to ensure communities still receive care, but they can only do so much. “Our community is suffering a lot,” she says. She is worried about burnout if funding isn’t restored.
Still, Agnes won’t rest until she has helped as many people as she can. Thanks to the support of the Rotary Club of Kampala, she recently went back to school and is working towards a degree in nursing. She hopes to learn new skills that will save even more lives.
“My dream is to make people feel good, to make them happy, and to give my service to the people,” says Agnes. “When you have positivity, nothing is impossible.”
The sky’s the limit
The Drone Didis are taking flight
Drones are helping rural women boost their income and India’s agricultural productivity.
I was excited to get a drone for my birthday last year. I couldn’t wait to get it into the air and see what my backyard looked like from the sky. But, as anyone who has used one can tell you, I quickly learned a harsh truth: Flying a drone isn’t easy. It takes a lot of practice and skill.
Maybe it’s time to pull the drone back out, because I was lucky to get a lesson from the experts last month in India. During my visit to Delhi, I met with Sangita Devi, Sumintra Devi, and Kajol Kumari—three Drone Didis from Bihar who are taking India’s agricultural productivity to new heights.
The women I met are part of the Indian government’s Namo Drone Didi program. (Didi is the Hindi word for “sister.”) It was launched in 2023 to help rural women boost their income and boost India’s agricultural productivity—and although the program is still in its early days, I’m already impressed by its results.
Right now, the Drone Didis primarily use their flying skills to fertilize crops. Applying fertilizer via drone has a lot of benefits over doing it by hand. Since you can spray farther away from the plant, the liquid fertilizer becomes more atomized—which means that it turns into finer droplets that cover more area. This benefits both farmers and the environment, because you need significantly less fertilizer and less water to help distribute it. Plus, it’s faster. One Drone Didi can cover as much as five acres in the same time it would take five people to cover half an acre.
I cannot wait to see how the program expands in the years ahead. The Indian government has plans to equip the drones with advanced sensors and imaging technology. This will allow Drone Didis to use real-time data to deliver targeted interventions to improve the quality and quantity of farmers’ crops. They will be able to detect diseases and pests, assess soil moisture levels, monitor crop growth, and more.
I’m equally excited to track how the Drone Didi program continues to empower women across India. Every Didi is affiliated with a self-help group, or SHG. The plan is to provide nearly 15,000 drones to SHGs across India by the end of next year.
In the United States, where I live, self-help groups are usually associated with mental health. In India, they’re a form of mutual aid. Each SHG is small—most are around 12 people, although some are as big as 25—and brings together women to support each other socially and financially. They pool their savings, access microloans at lower interest rates, and solve problems in areas like health and education.
The Didis I met with were longtime members of SHGs organized by JEEViKA, an organization in Bihar that works to lift people from rural areas out of poverty. During our time together in Delhi, Kajol told me about how JEEViKA helped her open her own shop three years ago, where she sells seeds and fertilizers. She loves being an entrepreneur, and when she was approached about becoming a Drone Didi, she knew it would do wonders for her business.
Each Didi attends a training program in Hyderabad or Noida, where they are taught how to pilot the drone and apply fertilizer effectively. (I was surprised to hear that learning to fly is apparently easier and takes less time than learning to fertilize!) Other women in their SHGs are trained as drone technicians, ready to repair the machines if any problems arise.
In the less than two years, the Drone Didi program is already transforming the lives of its pilots. Kajol is using the extra income she’s earned to expand her shop offerings and build a warehouse to store her stock. She also plans to send her children to a better school. Sangita’s family couldn’t afford a bicycle before she became a Drone Didi—today, she is the proud owner of an auto rickshaw.
Sumintra hopes that, when people see someone like her flying a huge drone, it changes their perception of what women are capable of. Like many women in her area, she married very young and was expected to stay home with her children. Today, her kids call her “Pilot Mummy” and dream about her flying airplanes one day.
I hope you think of the Didis the next time you hear the buzz of a drone above you at a wedding or a park. It’s remarkable how one piece of technology can reshape what is possible in a community. Kajol told me that people sometimes look at her and say, “She’s flying too high! What will she do next?”
Her response? “This is just the beginning. Wait and see what’s coming.”
Dora the plant explorer
She’s up at 3 a.m. to help farmers thrive
Dora Shimbwambwa looks for novel ways to fight invasive pests.

I’m an optimist by nature, but sometimes my optimism gets challenged. It’s not always easy to believe that the future is bright. Over the years, though, I’ve developed a trick that always helps cheer me up: I look to the unsung heroes who are doing amazing work around the world to improve people’s lives.
I’ve written about many of them in my Heroes in the Field series, and today I want to introduce you to another one. Her name is Dora Shimbwambwa, and she’s a plant researcher in Zambia who’s using her expertise to help farmers thrive in a warming climate.
Dora works as a research officer at the Zambian office of the Centre for Agriculture and Bioscience International, where she focuses on developing new ways to combat crop pests and diseases. Her research aims to help smallholder farmers improve their yields and incomes while promoting sustainable farming practices. As she explained, "My work involves creating awareness about crop pests and then researching different technologies that will help control the pest."
Dora seems to have been born to do this work, though it took her a while to realize it. She grew up at the Cotton Development Trust, an agricultural research station in southern Zambia where her father worked. Surrounded by plant scientists, she was exposed to agricultural science from an early age, but like a lot of kids, she didn’t pay much attention to her dad’s work.
When it was time to pick a career, she opted to follow in his footsteps, but mainly because she knew it would lead to a good job. Then, as she got into the work, she started to see the impact she could have for her community—“and from that time,” she says, “I haven’t looked back.”
Dora is especially focused on an invasive pest called fall armyworm, which has devastated maize crops across Africa in recent years. Unfortunately, climate change is making crops even more vulnerable—fall armyworm thrives in a hot, dry environment, and Zambia is in the midst of its worst drought in 40 years.
Synthetic pesticides are part of the solution, but they can be expensive, and they can kill other insects that are beneficial to the crops. So Dora is working on alternative methods, such as using biopesticides that target the fall armyworm specifically and don’t leave toxic residues.
Beyond her scientific expertise, what impresses me about Dora is her commitment to working directly with farmers and agricultural extension officers. She regularly travels to rural communities to conduct trainings and field trials, ensuring that her research translates into real-world impact. She keeps farmers’ hours—usually getting out of bed around 3 a.m., a habit she has had since she was a young girl.
Of course, none of this important work happens in isolation. Dora is quick to emphasize the collaborative nature of her research and acknowledge the people who have mentored her along the way. She's part of a growing network of African women in agricultural research, supported by organizations like African Women in Agricultural Research and Development. "Agriculture is mainly dominated by men,” Dora says. “So sometimes you just need a voice to guide you and give you confidence."
Thanks in large part to young scientists like Dora, I’m quite bullish about the future of African agriculture. By developing effective and practical ways to help farmers grow more food and earn more money, they are helping to build a brighter future for Africa. And that should give all of us reason to be optimistic.

Across the finish line
Makoy Samuel Yibi won’t stop until the world eradicates its next disease
Guinea worm once infected 3.5 million people every year. Thanks to heroes like Makoy, that number dropped to 13 last year.
When you see someone suffering from a terrible disease, it’s hard not to imagine a world where no one has to feel this way ever again. But the problem with eradication is that it’s really, really hard. The fewer cases remain, the more difficult it is to find them. That’s why, in all of human history, we’ve only eradicated two diseases: smallpox and the cattle disease rinderpest.
That might change soon.
The world is close to eradicating Guinea worm disease, a debilitating and painful condition that once devastated an estimated 3.5 million people in Africa and South Asia every year. Thanks to heroes like Makoy Samuel Yibi, that number dropped to 13 people in 2023.
As the national director of the South Sudan Ministry of Health’s Guinea Worm Eradication Program, Makoy helped reduce the number of cases in his country last year to just two. That’s a remarkable accomplishment by any standard, but it’s truly impressive when you consider the circumstances he and his team have faced: civil wars, the COVID-19 pandemic, the political changes brought by South Sudan’s decision to become an independent country in 2011, and the fact that the nation was once home to 90 percent of the world’s Guinea worm cases.
I recently caught up with Makoy at the COP climate conference in Dubai, where we both participated in an event focused on ending neglected tropical diseases, or NTDs, like Guinea worm. When you meet him in person, it’s hard to imagine a better person for the job. Makoy is passionate, brilliant, and laser-focused on making life better for the people of South Sudan. So I was surprised to learn that, as a young man, he never imagined a career in health.
Makoy was born in Terekeka County, a rural area located on the shores of the West Nile in southern Sudan. When he was a young man, Makoy had one primary focus: avoiding military service, which could be extremely dangerous. A chance meeting with a general from Terekeka resulted in a position with the national health department. A measles outbreak was ravaging parts of Sudan at the time, and Makoy’s first assignment was to travel from village to village providing care.
“What struck me,” he recalls, “was that, in every household we went to, we found at least half of the household was down with Guinea worm.”
The Guinea worm is a particularly nasty parasite. It’s unlikely to kill you, but the disease it causes—which is also called dracunculiasis, or “afflicted with little dragons”—can incapacitate you for months at a time and leave you permanently disabled. That can have devastating consequences if your family counts on you to grow the food you eat and sell it to make a living, as many people in South Sudan do.
The way the disease works is horrifying. If a person drinks water contaminated with Guinea worm larvae, the larvae enter the digestive system and mate. The impregnated female worm grows, undetected by the body’s immune system. Around a year later, the infected person will start to feel an itch somewhere on their body (usually the lower leg or foot). After a couple days, a painful blister appears and eventually bursts. The worm—which is now about one meter long—slowly starts to emerge from the wound.
This can take weeks or even months, and the pain it causes is excruciating. The wound can get infected, which could result in permanent disfigurement or even require amputation. And people often endure multiple worms emerging at the same time. Makoy has seen patients with as many as 40 worms.
And here’s the most insidious part: One of the few ways to relieve the pain of the blister is by soaking it in cold water, like a pond or a puddle. But that’s exactly what the worm wants. As soon as it touches water, it releases its larvae, starting the cycle anew. The Guinea worm is scarier and more efficient than any monster in a horror movie.
Makoy has seen countless times how devastating Guinea worm can be. “This is a situation where you see serious disruption of the livelihood of the community,” he says. “You see people going through a cycle of hunger because they don’t have enough. They have lost the window of cultivation. They’re not able to tend to their cattle, and there’s nothing they can do.”
There is no cure or treatment for Guinea worm, and yet, the world is on the doorstep of eradicating it. How? Through a series of highly effective interventions and a network of incredibly dedicated health workers.
Makoy’s team has built a network of volunteers in virtually every village in the country, who report rumors of Guinea worm cases. They spend every day searching for cases, getting the word out, and building trust in a country where more than 60 languages are spoken.
Makoy and his colleagues investigate every single rumor, no matter how remote. During the rainy season when the majority of cases happen, he often spends days hiking through the Sudd or up a mountain with all of his supplies on his back just to reach his destination. Last year, in a country the size of France with less than 100 miles of paved road, the team responded to nearly all of the 50,000 rumors they received within 24 hours.
Once the team finds a confirmed case, they make the patient as comfortable as possible and do what is called “controlled immersion.” This means soaking the affected area in a bucket of water and encouraging the worm to come out.
Makoy also spends a lot of time preventing people from getting Guinea worm in the first place. His team distributes free water filters and educates communities about safe water practices. The system they’ve built to support this work has strengthened health systems across the country, providing a platform for delivering other health services like childhood vaccination.
Makoy’s team has had a tremendous partner in all of this work: former U.S. President Jimmy Carter and the Carter Center. In 1995, when Makoy was first starting his public health journey, President Carter negotiated what remains the longest humanitarian ceasefire in history when he helped convince both sides of the Second Sudanese Civil War to lay down their arms and allow health workers access to treat Guinea worm and other diseases, like polio and river blindness. Today, the Carter Center continues to lead the global eradication campaign’s march to zero. The Gates Foundation is proud to support the Carter Center as part of our overall efforts to tackle NTDs. (You can learn more about Makoy’s partnership with the Carter Center in a new film called The President and the Dragon that is coming out later this year.)
Eradication is now within sight, although it won’t be easy to eliminate the last few cases. South Sudan previously reported no Guinea worm in 2018, but cases were subsequently discovered after a peace agreement was reached in the South Sudanese Civil War. And Guinea worm has recently been detected in dogs and other animals, mainly in Chad. Eradication will require stopping all transmission, both human and animal.
But Makoy Samuel Yibi is optimistic we can get there—and so am I. His determination to root out every last case makes me hopeful that we will someday soon celebrate the end of Guinea worm disease.
“In the places where Guinea worm has been eliminated,” he says, “you can actually see how communities have been energized. They are more active, and they are productive. The communities are now empowered to be more self-sufficient, because they don’t have to worry about Guinea worm.”

The life of Neandersquito
This scientist uses old insects to help fight malaria
Mara Lawniczak has an ingenious approach to studying mosquito evolution.
Of all the things I thought would help fight malaria, 100-year-old mosquitoes would not have been high on the list. Then I learned about the work of Dr. Mara Lawniczak.
An evolutionary geneticist at the Wellcome Sanger Institute in the United Kingdom, Mara has spent much of her career trying to understand how the genomes of various mosquito species have changed in response to humans’ attempts to kill them. When, where, and how fast has it happened? What does that say about how they might evolve in the future?
In recent years, genetics has become an increasingly important tool for fighting malaria. Because mosquitoes breed so fast (a female can lay thousands of eggs in her lifespan of a couple of weeks), they evolve rapidly, at least compared to humans. By studying their genes, researchers are able to understand things like how they develop resistance to insecticides, crucial information that helps humans stay one step ahead.
After a few years of studying mosquitoes’ genomes, Mara had grown frustrated by the fact that the only insects available for study were ones that had been captured recently. Without DNA from their ancestors, there was no way to know how their genomes had responded to decades of human attacks. “We were often saying, ‘If only we could look into the past,’” Mara says. “And then it suddenly struck me: I'm sure there are historical collections of mosquitoes around.”
She was right. The Natural History Museum in London has a collection of 34 million insects from all over the world, carefully collected and preserved. Among the collection is a large sample of mosquitoes dating from 1936, when a British entomologist named H.S. Leeson spent a year in East Africa capturing and cataloguing the insects in the hope of learning more about malaria. Leeson didn’t know it at the time—DNA wouldn’t be discovered until the 1950s—but his collection of mosquitoes would become a vast source of genetic material that someone like Mara could study.
Mara reached out to the museum’s curators. They wanted to help, but there was a problem: Extracting DNA from the insects would require Mara to grind them up. Since the museum’s mission is to preserve its collection for future generations, they couldn’t let her do that.
So Mara and her colleagues invented a way around the problem. Working with the museum’s team, they developed a novel way to extract DNA from mosquitoes without damaging the specimen.
They affectionately call this work Project Neandersquito. It’s not because the mosquitoes date from the time of Neanderthals, some 40,000 years ago—this isn’t Jurassic Park, where they extract dinosaur DNA from a prehistoric mosquito trapped in amber. It’s because the mosquitoes they’re studying are 1,000 or 2,000 generations removed from modern ones, just as Neanderthals are more than 1,000 generations removed from modern humans.
Mara’s team has made some surprising finds. For example, because mosquitoes started developing resistance to the insecticide DDT in the 1950s, they expected to see genetic mutations for resistance appearing around the same time. But they didn’t. “We still don't see them even as late as the 1980s,” she says. “So the mosquitoes were somehow making themselves resistant to DDT in ways that we still don't really understand.”
They also hope to get insight into what's coming. “How fast can mosquitoes evolve? And as we throw new control initiatives at them, how quickly are they going to get around them?” Other labs are now using the process devised by the Lawniczak Group to do their own research.
Project Neandersquito is just one of the ways Mara and her team are using genomics to advance the fight against malaria. A different project, the Malaria Cell Atlas, is providing new genetic data that could inform the effort to make better malaria drugs and vaccines. Another project is designed to make it easier and cheaper to identify a mosquito’s species using its DNA—it’s surprisingly hard to do just by looking—as well as whether it’s carrying the parasite that causes malaria, and even which species of the parasite it has. Ultimately, the project’s goal is to help governments get data that will help them get the most out of their anti-malaria efforts.
Mara would be the first to say that these are just a few examples of the tools the world needs to eradicate malaria. It’s going to take global cooperation from governments, the private sector, and academia. And now we can add natural history museums to the list.

Cool beans
Clare Mukankusi will make you geek out on beans
Beans are a staple crop in Uganda. This plant breeder is working to make them more nutritious and easier to grow.
What’s your favorite way to eat beans? Mine is in chili. I know that’s a controversial opinion in some parts of the United States, but in my family, we grew up eating bean chili. It was such a delicious, filling meal that I still enjoy today.
I’m a big fan of beans, but my love for them can’t touch Clare Mukankusi’s. She has devoted her whole career to creating more reasons to eat and love legumes.
Clare is a bean breeder in Kampala, Uganda. She works at the Alliance of Bioversity International and the International Center for Tropical Agriculture (or CIAT, from its name in Spanish)—which is part of CGIAR—where she spends her days developing new plant varieties that are more nutritious and easier to grow.
Like many Ugandans, Clare’s family has roots in agriculture. She grew up in Kisoro, a small town in the highlands of Uganda, where climbing beans are a major crop. Both her grandparents and her great-grandparents were farmers there, and Clare was proud to follow in their footsteps. She studied agriculture at Makerere University and later earned her Ph.D. in plant breeding from the University of Kwazulu-Natal before joining CIAT.
When it came time to choose a research focus, Clare didn’t hesitate. “At my home, beans are eaten on a daily basis,” she says. “And in most Ugandan homes, beans are on the table almost daily. They’re a major food in hospitals and schools.” The reasons why are clear: Beans are tasty and cheap. Plus, they’re a natural source of protein, carbohydrates, and other important nutrients.
But beans aren’t without their drawbacks. The varieties grown in Uganda can require as long as three hours of cooking time, and the cost of fuel is very high. Most people, including Clare, use charcoal and firewood to cook them, even if they have electricity at home. It’s just too expensive to use an electric burner for that long. But cooking with wood creates a lot of smoke, which causes health issues.
That’s where Clare’s work comes in. By using traditional crossbreeding techniques to create new varieties with desirable traits, she’s making beans easier to cook and more nutritious while still tasting delicious. For example, Clare is currently working on a variety that is ready to eat in as little as 40 minutes. It also has 15 percent more iron and 10 percent more zinc than a normal bean. Malnutrition and anemia remain big problems in Uganda, especially for children, and I am excited about how a crop like this could help kids stay healthy.
But Clare’s work isn’t only targeted at people who eat beans. She also wants to help those who grow and sell them. She is constantly thinking about the growing conditions farmers face, what types of soil they’re planting in, and even what kind of market they’re targeting. No one is going to buy a bean if it tastes weird or looks unappetizing. Clare has to stay up-to-date on what kind of products are most appealing in the places where her plants are grown.
The farmers she works with are worried about climate change, which is creating more extreme growing conditions and changing the types of pathogens they see in the field. “When it’s going to rain is no longer as predictable as it used to be,” she says. “It’s a challenge to keep up with the climate, pests, and disease. We need to be on the lookout for all of this to ensure that beans are able to survive even under different climates.”
This is a problem that farmers around the world are trying to adapt to, and Clare is working closely with bean breeders across Africa to make more climate-resilient beans. She’s a key leader in the Pan-Africa Bean Research Alliance, a consortium of 31 national research programs that facilitates information sharing and collaboration. Right now, Clare and her colleagues are focused on breeding qualities that make for better drought tolerance, like deeper roots that are resistant to root rot.
“Plant breeding is a really important science,” Clare says, “because it actually looks at how we are going to have food in the future. What food are we going to be consuming? Will we have enough food? We keep abreast with the population and changes in the behavior of people to make sure that we are actually addressing the needs of food at that time.”
The next time you eat a bean, I hope you think about Clare Mukankusi. It’s no exaggeration to say that her love of legumes will benefit millions of Ugandans. And her story is an inspiring reminder that even something as small as a bean can help people lead healthier, more fulfilling lives.

More than a job
For Eva Nangalo, saving mothers and babies is a calling
She’s a midwife, teacher, and advocate—and she’s changing childbirth in Uganda.
Officially, Uganda’s maternal mortality rate is double the global average. But because that number doesn’t count those who give birth at home—in a country where poverty, distance, stigma, and distrust are all barriers to medical care—Eva Nangalo believes the real one may be much higher.
That’s why, as a midwife determined to eliminate these deaths altogether, she’s spent the past 23 years working to make hospital deliveries both more safe and more common.
For Nangalo, this is more than a job. It’s her life’s work, and something she’s felt called to do for as long as she can remember. “I was created to be a midwife, born to be a midwife, trained to be a midwife,” she said. “It’s what is in my DNA. That’s what I am.”
Working the night shift at Nakaseke General Hospital in rural central Uganda and tending to her family’s farm while off the clock, Nangalo is known for sleeping maybe one or two hours, if that, a day. When the power goes out in the middle of a delivery—which happens often—she uses the flashlight on her cellphone to get the job done. She even keeps her hair short rather than style it the way she’d prefer.
In her own words: “I’ve wanted my hair to be like other women. But then I think of the one dollar saving a mother’s life.”
That isn’t theoretical. Nangalo regularly reaches into her own pockets to ensure that expecting mothers have the transportation they need to get to the hospital in the first place—and the food, milk, and medicine they and their babies need to survive not only childbirth but also what comes next. She once tore a piece of her own bedsheet to give to a mother who didn’t have one at home.
It’s no wonder she’s made a name for herself—literally—among the women she’s served, with many choosing to name their daughters after her.
Her advocacy efforts—and their effects—are broad and far-reaching. Understanding the fears and misconceptions that exist in Uganda around healthcare facilities, she uses the radio to reach skeptics and explain the merits of hospital deliveries and the higher risks of fatal infection and bleeding inherent to home births. She helped establish a newborn clinic in Nakaseke, improving the safety of childbirth at the hospital and increasing the number of families served. She even pushed the government to make good on its own policies and open a health facility in every sub-county.
It’s no exaggeration to say that Eva Nangalo is making childbirth in Uganda safer for everyone involved.
“The future looks bright,” one colleague said, “if we have more and more people like Eva.” Fortunately, she’s working to ensure that’s exactly what happens.
Statistically significant
Dr. Nonhlanhla Yende-Zuma is saving lives with math
She’s a statistician who faced impossibly long odds.
Growing up in a rural community with high rates of HIV and TB, Nonhlanhla Yende could have been just another statistic. Instead, she became a world-class statistician, one who’s using her expertise to save lives around the globe.
The name Nonhlanhla means “one with good luck” in Zulu, the most common first language in her native South Africa. But her rise from deep poverty to the head of biostatistics at one of Africa’s most prestigious research institutions had very little to do with luck. When I heard her story, I was blown away.
Dr. Nonhlanhla Yende-Zuma, as she is now known, was born in 1978, more than a decade before the fall of apartheid. Because her father left shortly after she was born, her family depended entirely on the small salary that her grandfather earned by raising cattle and working in the kitchen of a bed and breakfast. “My grandfather was working in a lovely kitchen for a white family,” she says, “but his own family often went hungry.”
Despite her hunger, Nonhlanhla had to walk 10 kilometers each way to the community’s one-room schoolhouse. Most people in her small town considered it a waste of time for a girl to attend school. “To this day, many people think that the only thing girls need to learn is how to do laundry and cook for their future husbands,” she says.
But Nonhlanhla imagined a different life for herself, largely because her Uncle Petros helped her see her own potential. From the time Nonhlanhla was very young, Petros pushed her to read anything he managed to find for her, and he became a fierce champion of her schooling. When her mother or grandmother told her to do a chore like fetching water, Petros would step in and say, “No, she’s studying.” He also stuck up for her when the boys in her class—and even some male teachers—tried to undermine the smart girl who was outshining the boys.
Nonhlanhla earned her “matric” (high school diploma) shortly after the fall of apartheid and then had an opportunity to attend the University of KwaZulu Natal (UKZN). Once she arrived, she signed up to study information technology, because she (and Petros) saw it as a pathway to a good career. But she felt lost and overwhelmed, and she was not the only one. She and a few other disadvantaged Black students approached a school counselor and acknowledged that they had no idea how to use a computer, and their limited command of English made it hard for them to understand their professors.
The counselor arranged for the students to get computer training, and she asked the professors to speak more slowly for the Zulu speakers. The counselor also suggested to Nonhlanhla that she might want to switch from IT to math. “That was a turning point. I was good in math, and math required very little English,” she says. (She is now fluent in English.)
After a year of earning top grades in math, she was invited to join a rigorous statistics course, which appealed to her because she felt statistics would give math more meaning in the real world. She excelled in the program and went on to become the first Black South African woman to graduate from UKZN with a PhD in statistics. And she did it while working full time and raising two daughters.
Nonhlanhla could have landed a lucrative position in the country’s prominent financial sector. Instead, she chose global health. She was drawn to the idea of working on the health challenges of her community and family.
When she was in high school, HIV/AIDS began to decimate her community. A few years later, a loved one died of AIDS. “No one could even use the term HIV or AIDS. They just said, ‘It’s that disease.’”
She began her global health career as an intern at CAPRISA, an organization that the Gates Foundation has long supported for its outstanding HIV research, and she has risen through the ranks. (A couple of years ago, I wrote about the married couple that founded CAPRISA.) Her work centers on assembling huge datasets and converting them into useful knowledge for clinicians and public health officials.
For example, when Dr. Yende-Zuma started at CAPRISA, clinicians had no idea how to treat patients infected with both HIV and TB. Most of the time, they gave these patients six months of TB treatments and only then initiated anti-retroviral therapies for HIV. Dr. Yende-Zuma and her colleagues produced strong evidence that this practice was resulting in needless deaths: Integrating TB treatment and ARVs reduced mortality drastically. Their evidence was so compelling that the World Health Organization adopted this guidance for doctors around the globe.
As you can imagine, Dr. Yende-Zuma’s skills were in great demand when COVID arrived in South Africa. Her husband and two children saw very little of her for the first year of the pandemic, because she worked long hours providing support to people who were advising the national health department. For instance, she designed an implementation study to determine whether the not-yet-approved Johnson & Johnson vaccine would be effective in South Africa; there was good reason to worry that the country’s high HIV prevalence could reduce the vaccine’s effectiveness. She and her colleagues proved that the vaccine was, in fact, highly effective.
She also helped many people in her community overcome their skepticism of Western medicine. “There were lots of rumors about the vaccine. I told my mom, ‘Tell your church ladies that your daughter was part of the team that brought those vaccines to South Africa and proved they were safe and effective,” she says. Dr. Yende-Zuma became a fixture on television, bringing the same message to the whole country. “In my wildest dreams,” she says, “I never thought I’d be part of a high-level team who would do something so important for our country.”
If she hadn’t been so determined—and encouraged by her uncle—she might never have had the chance. Instead, she’s advancing health policy and practice around the world, while helping many others make the most of their talents too.

Growing around grief
Wendo Aszed’s best friend died. Then she did something remarkable.
Now she and her team provide services for women and girls throughout rural Kenya.
As a child growing up in the 1980s on a small farm in western Kenya, Wendo Aszed found it difficult to make good friends. She finally found a confidant when she was in her twenties and working at a bank in the city of Nakuru, Kenya. Her friend was a smart, kind man who became someone “I would die for,” Wendo says.
In 2007, he told her that he had just tested positive for HIV. Wendo immediately got to work trying to help him get lifesaving anti-retroviral medication (ARVs). But by that time, her friend had already contracted meningitis, and he died less than a month later. “When you have the kind of grief I felt, you might grow around it, like a tree grows around a rock,” she explains. “But you never, ever lose it.”
In the hope of saving others from the same fate, Wendo started visiting nearby villages and engaging women in wide-ranging conversations about their health and lives. Eventually she was able to build enough trust to offer gentle advice on how they might find help for addressing their biggest challenges—from HIV infection to the loss of young children at the hands of abusers in the community.
Wendo was so passionate about this mission that, in 2009, she quit her financially secure job at the bank and began helping the women full time. “I had no formal training for this, and I had absolutely no savings to do it, but I just had to do it,” she recalls. She recruited a group of mentors from the local nonprofit community and set up an organization, which she called Dandelion Africa—a tribute to the resilience of women thriving in difficult environments. Dandelion Africa is how Wendo grew around her grief.
The first two years of operations almost broke her. She had no grant money or other resources to pay herself or anyone else. “Ironically, I felt selfish doing what I was doing,” she says. “I knew I was helping these women, but our family was going through hell. My husband did his best to support us with his earnings as a farm manager, but we barely had enough to pay school fees for our children.”
Just when Wendo was about to give up, the Kenyan government gave Dandelion Africa its first grant—a total of $3,500. The grant allowed Dandelion to provide HIV testing and counseling to almost everyone in one community. Through this work, Wendo learned just how many people living with HIV had no medical or psychological support. She saw that she had to go upstream—that is, not just ensure that women could get ARVs but also help change the economic and social conditions that were leading to such high rates of transmission.
Even as she started to line up the resources to go upstream, Wendo faced significant obstacles because of her gender. Once, when she sat down with a local official as she was organizing a government-funded free health clinic for his community, he started to tell her that she would have to pay for the doctors’ and nurses’ gasoline, the staff lunches, and washing the uniforms. When she resisted, he stood up and said, “In my tribe, when a woman speaks like that to a man, we slap her.” Wendo replied: “In my tribe, when a man hits a woman, we kill him.” The official sat down and said, “Okay, let’s plan this clinic.”
Over the subsequent decade, Dandelion built an all-Kenyan staff and a network of more than 200 volunteers, providing comprehensive health, economic, and educational services across a large swath of rural Kenya. Today, Dandelion Africa provides one of the best examples I’ve seen of community-led problem solving.
She and her team built—partly with their own hands—the all-hours Dandelion Medical Centre. The facility, which opened three years ago, is now driving down maternal mortality, HIV transmission from mothers to their babies, and vaccine-preventable diseases in a region where families previously had little access to even the most basic care. “When I first started the organization, I was barely staying alive,” Wendo says. “To come full circle and open a medical center that ensures every woman in the region can get quality care, that was just overwhelming to me. I just wish my best friend could have been with us at the opening.”
Dandelion Africa is also taking primary care directly to families. Its nurses hop on motorbikes and travel to homes, where they provide immunization, HIV testing, and other services. Dandelion Africa has also helped thousands of women and girls access contraceptives and sanitary supplies for the first time.
Wendo’s organization has also launched efforts to empower women and girls. For example, it helps women access small loans for starting their own businesses. It helps women adopt profitable farming techniques. And Wendo’s 22-year-old son helped create a successful effort to engage men and boys as advocates for women and girls. “When I see men becoming champions fighting FGM and whole villages saying no to FGM because they see how it harms the whole community, I know we’re doing something right,” Wendo says.
Counterintuitively, Wendo often finds it even more difficult to change women’s perceptions than men’s. “Sometimes, the women simply can’t imagine what it would be like not to be beaten by their husbands,” she says. “But we’ve learned how to reach them. We share stories that help them envision a different path.”
While the name Dandelion Africa suggests that Wendo has aspirations to expand in other parts of the continent, that is not the case. “We are going to stay in the hardest parts of Kenya, where no one else wants to work,” she explains. To achieve greater scale, she is working to cultivate 50 more dandelion-type leaders around the country.
Although finding 50 others with Wendo’s drive will not be easy, I’m optimistic that this tough, resilient leader will succeed.

True grit
Malaria is deeply personal for this Kenyan scientist
Losing a brother to the disease supercharged her fight against malaria.
I know a lot of people who are driven to do something. When we were in high school, for example, Paul Allen and I would get quite absorbed in software projects—including neglecting sleep and showers. But that pales in comparison to the determination of Dr. Damaris Matoke-Muhia, a leader in the fight against malaria and other mosquito-borne diseases.
Damaris grew up in Birongo, Kenya, a rural village in the country’s western highlands. She showed remarkable talent in math and science from an early age, but she experienced discrimination at school and in her community because of her gender. Even some extended family members couldn’t understand why the family would “waste” (as they put it) precious resources on Damaris’s school fees, given that most girls in her village got married early or dropped out before completing secondary school.
Despite the social pressures, her father, who was a schoolteacher, was adamant that Damaris continue her studies. After Damaris graduated from secondary school, her father sold cows and a plot of land to pay for her tuition at the University of Mysore, in India. But he could afford to send her only $50 every three months for rent and living expenses. So five days a week, Damaris walked more than 15 miles to the university and back, and she barely ate enough to survive. “If I couldn’t eat a meal at a friend’s house, I would often go two days without eating,” she says. “But I refused to break, and I never missed a class.” She entered university weighing about 150 pounds, and when she finished her studies in India, she was down to only 90 pounds. Many neighbors assumed she had contracted HIV/AIDS. “They ridiculed my father. They said, ‘You spent all that money, and now she comes home to die.’”
On top of deprivation, Damaris suffered a huge loss while she was studying in India. She was 23 and working on a master’s degree in biotechnology when her younger brother Abel, also a gifted science student, died of an especially dangerous form of malaria. Damaris couldn’t afford a ticket home for the funeral services.
Abel’s death had a profound effect on Damaris’s life, giving her clarity on how she would use the education for which she and her parents had sacrificed. “For the first time, I knew my education was not a mistake or a waste,” she explains. “I knew I could play a role in eliminating malaria in my home country.”
After returning to Kenya, Damaris took on an almost-impossible load again. While pursuing a doctorate in molecular medicine, she also worked full time as a research officer at the Kenya Medical Research Institute (KEMRI) so she would have money to help put her seven surviving siblings—including three girls—through university. Thanks to her support, all seven earned undergraduate degrees, and two went on to complete post-graduate degrees as well.
Today, Dr. Damaris Matoke-Muhia is Principal Research Scientist at KEMRI and is manager for the Capacity Building, Gender Mainstreaming, and Career Progression program at the Pan-African Mosquito Control Association. In the field, she traps mosquitoes to study their behavior and learn how they develop insecticide resistance. In the lab, she is researching new techniques to counter this resistance and specific innovations to control malaria. In villages across Kenya, she surveys breeding sites, investigates the effectiveness of preventive tools, conducts health education for families, and screens for malaria infections. On the international level, she is helping women rise to leadership positions in the fight against malaria and other mosquito-borne diseases.
Her focus on women is not just a function of the gender discrimination she faces to this day. It’s also driven by the knowledge that the world has been trying to fight malaria with one hand tied behind its back.
Research demonstrates that men hold 75 percent of all leadership positions in global health—even though women perform 70 percent of all healthcare services worldwide and, perhaps even more important, hold the key to implementing effective malaria control measures at the household level. “Women are clearly in charge in the villages I travel to for field work,” Damaris says.
This is why our foundation is supporting Damaris’s work to open the doors to women in community-level initiatives and senior positions in international health organizations. As Damaris says, “If we’re serious about malaria elimination in Africa, women must help develop, design, deliver, and implement strategies that take account of the reality that women are in charge of ensuring things go well at the household level.”
Damaris and her colleagues have researched the major obstacles that make it hard for women to take top leadership roles, and now they’re addressing each one. For example, they are providing leadership training to women in science, helping rising leaders find mentors, and advocating for workplace policies that support women.
Damaris offers multiple reasons for optimism. For example, she will soon be able to use her networks of women leaders to help deploy RTS,S—the world’s first malaria vaccine. Other effective control measures include improved insecticide-treated bed nets and attractive targeted sugar baits. In combination, these new tools will prevent tens of thousands of children from getting malaria each year. They will also help free mothers to focus on things other than taking care of family members suffering with malaria—giving a big boost to their productivity at home and in the workplace.
Her greatest source of optimism is her own children. In addition to having a 10-month-old son, she and her husband have two daughters, ages 13 and 10, who are outstanding science students and want to pursue health as a career. Their older daughter, Amirah, wants to be a neonatologist. Their younger daughter, Anabel, wants to be a veterinarian. Thanks to their parents and their community of friends in Nairobi, neither girl sees any reason to limit her dreams.

Pathogen prevention
In Africa, detecting disease outbreaks before they become a global threat
Using genomic sequencing technologies, this hero is working to prevent the next pandemic.
While promoting my new pandemic book the last month, I’ve been telling audiences and interviewers that if we want to make COVID-19 the last pandemic, we need to combat infectious diseases the same way we fight fires.
Just like we have a robust system of fire alarms, firefighters, and fire hydrants to help detect and extinguish fires, we need to create an equally effective system to identify and respond to new disease outbreaks.
This firefighting comparison is also a useful way to understand the amazing work of Sofonias Tessema.
Officially, Sofonias is the program lead for the Africa Pathogen Genomics Initiative at the Africa Centers for Disease Control and Prevention or Africa CDC. But in firefighting terms you might think of him as a fire safety officer who is building a network of fire watchtowers and smoke detectors across Africa.
Instead of looking out for the first signs of a fire before it can spread, however, Sofonias is focused on quickly detecting deadly pathogens before they can grow into a global threat. And instead of using watchtowers and smoke detectors, he relies on powerful genomic sequencing technologies to spot disease outbreaks.
Genomic sequencing allows scientists to read the DNA and RNA of pathogens and understand what they are, how they spread from one person to another, and develop counter measures like vaccines. During COVID-19, this technology has been an invaluable tool for identifying new variants, tracking the evolution and spread of the virus, and guiding public health responses.
Advances in this technology have made it easier, faster, and cheaper to do genomic surveillance. Over the last two decades, the price of sequencing a full human genome has fallen dramatically. And one company, Oxford-Nanopore, has even developed a portable gene sequencer that can be operated with a laptop and no need for a lab, allowing health officials to conduct genetic testing in remote areas where outbreaks may occur.
As powerful as genomic sequencing technologies have become, many countries have not taken full advantage of them. Building genomic disease surveillance capacity presents challenges because it requires investments in labs, expensive equipment, and specially trained personnel. While the COVID-19 pandemic has sparked new interest in using genomic sequencing to improve disease surveillance, many parts of the world are still working to strengthen their capacity to use this critical technology.
In 2019, Sofonias joined the Africa CDC to establish a continent-wide genomic disease surveillance network. One of Sofonias’s first projects was to conduct an assessment to understand how many African nations were prepared to use this technology.
The results, Sofonias said, were shocking.
Of the African Union’s 55 member states, just seven had public health institutions with trained personnel and equipment to do genetic sequencing.
Given the scale of the job before them, Sofonias and his team had planned for a phased approach to help African nations build genomic surveillance capabilities. They had to acquire the technology, hire and train the technicians to operate them, and create the data systems so governments can analyze and share the genetic information and use it to inform public health decisions. Building this system would take time.
But the Africa CDC soon learned that time was a luxury they didn’t have. Within weeks of Sofonias joining the Africa CDC, the first cases of COVID-19 were detected in China. And two months later, the first cases were identified in African countries.
It’s hard to overstate the challenge before Sofonias and the Africa CDC. While genomic surveillance had been used during Ebola, Lassa fever, and cholera outbreaks, bringing this technology to scale posed many challenges in Africa, where many countries did not have the infrastructure or trained personnel to run these labs.
But this was just the kind of challenge Sofonias had always been eager to take on.
Born in Ethiopia, Sofonias grew up in a rural town where malaria was always a major threat. Seeing people die and suffer from the mosquito-borne disease got him interested in a career in public health. He earned a PhD in malaria genomics, an emerging field of research that uses genetic data of the malaria parasite to advance malaria eradication efforts. After graduate school, he was working as postdoctoral fellow at the University of California in San Francisco, where he was focused on how genomic data combined with mobile phone data could help researchers understand how malaria spreads from one country to another.
In 2019, when a call came from the Africa CDC asking if he would use his knowledge of genomic surveillance technologies to help Africa, he jumped at the opportunity. Sofonias saw the untapped potential of this new technology to make more informed public health decisions in Africa. And after years living abroad, he was also excited to return home to Ethiopia, where the Africa CDC is based.
Sofonias and his team scrambled to quickly build up Africa’s capacity to do genomic disease surveillance. The Africa CDC focused first on scaling up COVID-19 testing capabilities. At the beginning of the pandemic, only two African nations had the ability to perform PCR COVID tests, highly accurate tests that detect genetic material from the virus.
At the same time, his team worked to acquire next-generation sequencing technologies (NGS) for Africa. NGS technologies offer a more efficient, accurate, and cheaper way for researchers to track the slightest genetic changes in pathogens which may cause disease outbreaks. This effort received support from a group of public, private, and non-profit partners including the African Union, Illumina and Oxford Nanopore, which produce next-generation sequencing machines, the US Centers for Disease Control and our foundation.
Thanks to Sofonias and the rest of the Africa Pathogen Genomics Initiative team, 31 African nations now have the capability to do genetic sequencing for surveillance of COVID, malaria, cholera, Ebola, and other diseases.
Despite this progress, much remains to be done. Sofonias’s team faces challenges in bringing this technology to all African nations. Access to the equipment needed in the labs has been delayed because of global supply chain disruptions. Training enough lab technicians and data scientists to process and analyze the samples has been difficult. Finally, more coordination is needed between countries to share their genetic data and use it to inform collective health responses.
But every month, Sofonias’s team continues to strengthen and expand the system across the continent. The goal is to create a seamless, integrated network that includes laboratories at the community level, which can spot the first signs of an outbreak, perform genomic testing of pathogens, and analyze the results to guide a public health response.
“Our vision is bold. Our vision is optimistic. We always push forward and continue to work with the countries to show that this is actually feasible,” he said. “It really makes me hopeful that this technology can improve outbreak detection and response in Africa.”
Sofonias shared the progress and challenges of building a genomic disease surveillance network with a group of graduate students who participated in a recent Gates Notes Deep Dive on pandemic prevention.
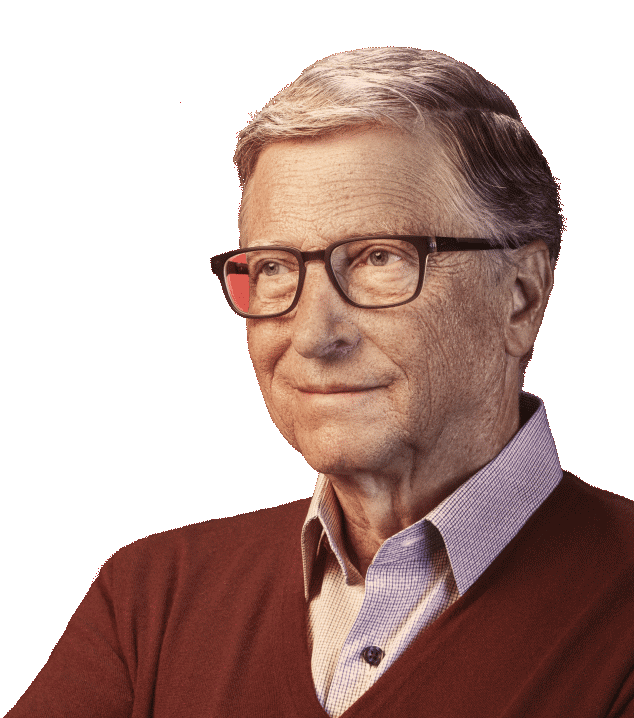
Pioneering research
She helped change vaccines forever
Long before most of us heard of mRNA vaccines, this hero saw their potential to save lives.
For most people, the highly effective mRNA COVID vaccines made by Moderna and Pfizer-BioNTech seemed to come out of the blue. But these new vaccines, which were essential to end this pandemic and will likely play a critical role in preventing future pandemics, are the product of decades of painstaking work by researchers.
One of those researchers is Dr. Katalin Karikó, a Hungarian biochemist who long ago saw the potential of mRNA to save lives when few others did.
The daughter of a small-town butcher in Hungary, Karikó knew from a young age that she wanted to become a scientist. She was drawn to biochemistry and developed a particular fascination with messenger RNA, or mRNA, molecules that (among other things) direct the creation of proteins in your body.
Messenger RNA functions as a kind of middleman—it carries the directions for making proteins from your DNA to the factories in your cells where the proteins will be assembled. It’s a bit like the waiter in a restaurant who writes down your order and takes it to the kitchen, where the cooks will make your meal.
In the 1980s, while working on her PhD in her native Hungary, Karikó became convinced that tiny strands of mRNA could be injected into cells to send instructions to the body to make its own medicines. She was interested in developing mRNA treatments for stroke, cancer, and other diseases.
Although vaccines were not the focus of Karikó’s work, other researchers saw that it would be possible to use mRNA to make those as well—for flu, coronaviruses, and maybe even various forms of cancer.
Using mRNA to make vaccines would be a major departure from the way most vaccines work. Many conventional vaccines operate by injecting a weakened or dead form of the virus you’re trying to stop. Your immune system sees the new shapes on the virus, kicks into gear, and builds up immunity. While conventional vaccines have been very effective, it takes years of lab work and clinical studies to make sure that they are safe and will produce a good immune response.
The idea behind mRNA vaccines was quite clever. Since mRNA takes the orders for proteins from the DNA and delivers them to the cooks in your cells’ kitchen, what if we could change those orders in a very targeted way? By teaching your cells to make shapes that match shapes on the actual virus, the vaccine would trigger your immune system without having to introduce the virus itself.
If they could be made, mRNA vaccines would be a huge advance over conventional vaccines. Once you had mapped out all the proteins that make up the virus you wanted to target, you’d identify the one that you want antibodies to grab. Then you’d study the virus’s genetic code to find the instructions for making that protein, and you’d put that code into the vaccine using mRNA. If, later, you wanted to attack a different protein, you’d just change the mRNA. This design process would take at most a few weeks. You would ask the waiter for fries instead of a side salad, and your immune system would do the rest.
There was just one problem: It was only a theory. No one had ever actually made an mRNA vaccine. What’s more, most people in the field thought it was crazy to even try, not least because mRNA is inherently unstable and prone to degrading quickly. Also, cells have evolved to avoid being hijacked by foreign mRNA, and there would need to be a way of getting around this defense system.
Karikó’s interest in mRNA eventually brought her to the U.S. And in 1993, while doing research at the University of Pennsylvania, Karikó and her boss managed a feat that told them they were on to something: They got a human cell to produce a tiny amount of new proteins using a modified version of mRNA that had been altered so it could get past the cell’s defense system. This was a breakthrough, because it meant that if they could expand the production dramatically, they would be able to make a cancer treatment using mRNA.
Stories of medical discoveries often don’t travel in straight line from breakthrough to lifesaving impact. And Karikó’s story is no different. Karikó’s work lost momentum when her boss left academia for a biotech firm. She no longer had a lab or financial support for her work; although she applied for grant after grant, every application was rejected. In 1995, she had a cancer scare, she was taken off the tenure track at work, and her husband was stuck in Hungary because of a problem with his visa. But Karikó was undeterred.
Then in 1997, she began working with Drew Weissman, a new colleague who came to the University of Pennsylvania with a promising background: He had done a fellowship at NIH under the supervision of Tony Fauci, and he was interested in using Karikó’s work on mRNA to develop vaccines.
Together Karikó and Weissman kept pursuing the idea of working with mRNA that had been engineered in a lab. But they still had to get more mRNA past the cell’s defense systems, a problem that other scientists helped solve. In 1999, a cancer researcher named Pieter Cullis and his colleagues proposed that lipids—basically, tiny bits of fat—could be used to encase and protect a more delicate molecule, such as mRNA. Six years later, working with Cullis, biochemist Ian MacLachlan did it for the first time. The lipid nanoparticles he developed paved the way for the first mRNA vaccines.
As late as 2010, hardly anyone in the federal government or private industry was interested in trying to make vaccines using mRNA. Major pharmaceutical companies had tried and failed, and some scientists felt that mRNA would never trigger enough of a response in the body. But an official at DARPA, the little-known research program for the U.S. military, saw enough promise in the technology that he started funding mRNA vaccines for infectious diseases.
As pioneering as this work was, it didn’t lead immediately to new vaccines. Accomplishing that would be the task of companies dedicated to translating the breakthrough into a product that could be approved and sold; the U.S.-based Moderna and Germany-based CureVac and BioNTech were founded to do just that.
In 2014, Karikó joined BioNTech, which was working on an mRNA vaccine for cancer. Early efforts didn’t work, although a test of a rabies vaccine showed promise. Still, Karikó and her BioNTech colleagues persevered, as did scientists at Moderna. When COVID hit, they immediately set out to make a vaccine for the new virus. It was a good bet.
The notion that mapping a virus’s genome would allow you to create an mRNA vaccine in a matter of weeks proved to be exactly right. In March 2020, just six weeks after scientists sequenced the COVID virus’s genome, Moderna announced that it had identified an mRNA-based candidate and begun making it for clinical trials. On December 31, the mRNA vaccine made by BioNTech in partnership with Pfizer was approved for emergency use by the World Health Organization. When Karikó received the first dose of the vaccine she had done so much to create—a few days before it was officially approved—she wept.
For all her amazing foresight, I doubt even Dr. Karikó imagined that mRNA vaccines would one day play an essential role in ending a pandemic – and giving us a tool to prevent the next one. And to me, that’s the important lesson of her story: It’s impossible to predict exactly how breakthroughs will shape the future. That’s why it’s critical, if the science makes sense, that we should be willing to bet on crazy sounding ideas and the researchers like Dr. Kariko willing to fight tooth and nail to pursue them. They just might change the world.

Uplifting education
Inspiring girls to believe in themselves
This hero’s school empowers girls to see their potential for greatness.
As a middle school student in India, Sudha Varghese was paging through a magazine when she saw a photo that changed her life. It was a picture of a ramshackle hut on a roadside in Bihar State. This was where some of India’s poorest families live, a caption explained.
The image stuck with her. Raised in a prosperous family in Kerala, India, Sudha couldn’t imagine living in such conditions. Something, she thought, needed to be done to help the poor. And she decided she would be the one to do it.
“I decided all my efforts, all my resources, all my time, all my love, whatever I have, all that will go for the poor people who are needy,” she said.
Sudha’s family didn’t support her plans. But she didn’t give up. She joined a religious order, became a Catholic nun, and started doing charitable work. A few years later, disappointed that she wasn’t doing enough to help the poorest, Sudha struck out on her own. She moved to Bihar to live in a community like the one she saw in that photograph.
The people who lived there, she learned, were the Musahar. Musahar literally means “rat eaters.” In India’s earlier caste system, they were viewed as the “untouchables.” They could not own land and worked as poorly paid farm laborers. Most never had the opportunity to go to school. (You can read more about my visit in 2010 to a Musahar village in India here.)
Sudha asked some Musahar villagers for a place to stay. They offered her a grain shed. And so began a lifetime of work to improve their lives.
Sudha focused her efforts on the Musahar women and girls. They suffered from discrimination, and often violence. Sudha worked with them so that they could stand up for their rights. She helped them get funding for hand pumps so they could have access to clean water. She also encouraged them to ask for higher wages.
But the biggest challenge Musahar women faced, Sudha says, was how they had come to see themselves. Entering a room, they would look at the ground and always take a back seat. They thought they were not worthy of respect, she said.
Changing mindsets is never easy. And while she could work with the adult women, it was even more important to work with girls, she decided. They needed an education in a school that would help them redefine their self-image by believing in themselves and their potential for greatness.
No school like that existed, so Sudha decided to open one herself. She named it Prerna, which means “inspiration” in Hindi.
Prerna school offers reading, writing, math, history, and science. But Sudha wanted her students to learn how to stand up for themselves and be confident. So, she also added karate to the curriculum. The girls proved to be talented martial artists. Some have even competed in the world karate championships in Japan.
Sudha also teaches them yoga, drawing, painting, and singing. Her goal is to create well-rounded young women ready to pursue their dreams. More than 5,000 girls have graduated from her program.
During COVID-19, her school, like all schools in India, was forced to close for many months. Sudha and the other teacher tried to stay in touch as best they could through online classes, although many girls didn’t have access to mobile phones. They are in the process of restarting in-person learning this year.
Sudha also runs Nari Gunjan (“woman’s voice”), a nonprofit organization that provides education, literacy, vocational training, healthcare, and life skills for these women and girls in Bihar.
There is still much more work to be done to improve the lives of this community. Many families still live in poverty and are marginalized. But thanks to Sudha’s school and many efforts being made by the Bihar Government, Musahar girls are now pursuing their dreams of studying to become doctors, engineers, lawyers, and leaders in their community.
If a photographer came to Bihar today, a photo of a hut by the side of the road, like the one Sudha saw in a magazine decades ago, wouldn’t capture the story of the Musahar. What would, is a portrait of the young graduates of Sudha’s school. It would show them holding their heads high, looking straight into the camera’s lens, and inviting anyone who ever doubted themselves to believe in their own potential.

Challenging tradition
Her dream is freedom for women and girls
This hero’s community is being transformed by the girls who attend her school.
As a girl growing up in rural Kenya, Kakenya Ntaiya learned from an early age that her future had already been decided for her.
By age 5, according to local Maasai custom, she would be engaged to be married. By 13, she would go through female genital mutilation/cutting (FGM/C) and leave school to become a wife and mother. Her days would be filled with chores, fetching water, collecting wood, cooking, and cleaning. And she would be expected to raise her daughters to follow the same path.
But Kakenya had a different plan for her future—and the future of her community.
She was determined to stay in school and become a teacher. At age 13, when she was about to be pulled out of school and undergo FGM/C she made a deal with her father: She would submit to cutting, but only if she could continue with her schooling. Her father agreed.
It’s hard to overstate the courage it took for Kakenya to defy local traditions. While FGM/C has been illegal in Kenya since 2001, the practice persists in rural communities because many families believe it will improve their daughters’ chances of finding a husband. Kakenya endured the painful cutting ceremony, but she was able to avoid marriage and stay in school. She won a full scholarship to attend college in the United States and went on to earn a PhD in education.
She founded Kakenya’s Dream, an international nonprofit organization dedicated to educating girls and ending harmful traditional practices like child marriage. She returned to her home village to work with the Maasai elders in her community. She convinced them that girls—not just boys—should have access to education. In 2009, she opened Kakenya’s Center for Excellence, a school for girls built on land donated by the elders.
Kakenya’s school enrolls girls starting at age 10, when parents are likely to start pulling their daughters out of school to get married. Students get housing, uniforms, books, and a strong education. In return, parents agree to not have their daughters get married or undergo cutting while they are in school. As part of Kakenya’s program, she also runs programs for Maasai boys and community members, helping them understand how child marriage and genital cutting harm girls and their entire community.
“All of it is about breaking the silence and that has really helped us to break through all these cultural barriers that hinder women,” Kakenya said.
Graduates of Kakenya’s school have gone on to college in Kenya and study abroad. Like Kakenya, many return to help their communities. One recent graduate now studying nursing in Australia, for example, used her school break to volunteer at a local health clinic in Kenya.
I first heard about Kakenya through Melinda when she was working on her book, The Moment of Lift: How Empowering Women Changes the World. Her story is a powerful example of how one person’s act of bravery can spark dramatic change not only in their own life but also in hundreds of other lives.
Kakenya’s experience fighting for change is also a reminder of the work that needs to be done to improve the lives of women and girls. Over the last two decades, our foundation has been dedicated to reducing inequity around the world—in health, education, and opportunity. But it became increasingly clear to us that something was standing in the way of these efforts: In many ways, women and girls were being undervalued.
That’s why in 2020, our foundation officially launched a Gender Equality Division to further our commitment to gender equality outcomes across the UN’s Sustainable Development Goals. The new division is working to ensure gender equality is incorporated across the foundation’s work. Gender equality initiatives include women’s economic empowerment, women in leadership, data and evidence, and innovation in science and technology to improve women’s health. As part of this work, we have supported the Child Marriage Learning Partners Consortium and continue learning more to fill gaps in knowledge of child marriage, its drivers, and solutions.
When you look closely at the data, you see how gender inequality complicates the fight against poverty and disease. Just consider the impact of COVID-19. The pandemic has had an intense impact on women. New data shows that the pandemic has led to disruptions to women’s health services, job losses in sectors where women are overrepresented, and a sharp increase in caregiving needs and other unpaid work.
The pandemic has created new challenges for the girls at Kakenya’s school, too. During the COVID lockdown, Kakenya’s school was forced to shut down and the girls were sent home. For Kakenya, the pandemic was a critical test of her school’s curriculum. She had taught her students how to be independent and stand up for themselves. But when they returned home for many months, the girls would be under pressure from their families to get married, often out of economic hardship that was exacerbated by the pandemic.
Early pregnancy and marriage are on the rise around the world and it’s still a massive problem in Kenya. Fortunately, at Kakenya’s school, all the girls returned. None had undergone FGM/C. None had gotten married.
“This community is being transformed by the girls that have gone through our school,” Kakenya said.

Heroic acts
Meet the heroes in Africa fighting back against this pandemic—and working to prevent the next one
As Africa faces many challenges during the pandemic, these heroes are making a difference.
In Africa, the latest statistics on COVID-19 are discouraging. Just 6 percent—about 78 millionof the continent’s 1.3 billion people have been fully vaccinated. Worldwide, by comparison, 43 percent are fully vaccinated, and boosters are now widely available in many countries.
Without enough vaccines available in Africa, COVID-19 marches on infecting millions of people. Even assessing the true scale of the pandemic on the continent is difficult. A recent World Health Organization assessment estimated that only one in seven cases of COVID in Africa are being detected because of a limited amount of testing.
And while many Western and Asian countries are recovering economically from the pandemic and returning to some version of normalcy, most countries in Africa continue to struggle. Disruptions to schooling, health care, and livelihoods have sunk many families deeper into poverty, leaving them without enough food and basic services.
We should all be upset about this inequity. (I’ve written recently about this divide and the steps the world needs to take to get the virus under control.) It’s critical that more be done to get vaccines into the arms of the people at high risk for COVID, including the elderly and immunocompromised, who are living in low-income countries. And the recent detection of the Omicron variant serves as a reminder of how important increasing vaccination rates is to deter new mutations of the virus from emerging.
But even during this difficult time, I think it’s important to highlight the many Africans who are fighting back against this pandemic. They are stepping up to alleviate suffering, to combat misinformation, and to develop the tools needed to prevent future pandemics.
There are thousands of examples of heroic work being done in Africa during this pandemic. Here are three stories of organizations and individuals who are working to save lives and bring hope to their communities.
1. South Africa: The Truck
As COVID-19 swept across South Africa, one of the most pressing needs was access to public health information. People needed to know about the virus and how to stay safe. And as South Africa started rolling out COVID vaccines this year, health officials were also tasked with counteracting the spread of misinformation about the virus and vaccines. This was especially challenging in hard-to-reach communities in South Africa, where people don’t have access to television and other media. But UNICEF, in partnership with the national government, had an answer to this challenge: A truck. Not just any truck but a multi-media messenger on wheels. The truck has LED screens, which allows the truck’s organizer to broadcast videos telling local stories about COVID-19. They also organize presentations in communities to raise awareness of the virus, teach people how to prevent its spread, and promote COVID testing and vaccinations. The truck has logged more than 40,000 miles and delivered messages to hundreds of thousands of people.
2. Lesotho: Mamello Makhele
Mamello Makhele is a nurse-midwife working to improve health care for women in rural Lesotho, where there are high rates of maternal mortality. During the pandemic lockdowns many health facilities closed, leaving women living in these remote communities without access to family planning services. On foot and by donkey, Mamello travels high into the mountain to offer health care, deliver babies, and distribute contraceptives. Mamello has also worked nationwide to empower young women, encouraging them to take control of their health and prevent unwanted pregnancies. Thanks to her incredible work, many women are healthier today in Lesotho.
3. Tanzania: Afyadata
Even as the world seeks to end the current COVID-19 pandemic, we need to also be thinking about how to prevent future pandemics. That’s just what a mobile app called Afyadata is helping health officials do in Tanzania. Designed by the Southern African Center for Infectious Disease Surveillance (SACIDS), Afyadata is a digital surveillance tool that allows health workers and even ordinary people to serve as disease detectives. Users can report unusual health occurrences not only in humans, but also animals. Monitoring animals is critical because most new pathogens start in animals before they spread and sicken humans. With the app, farmers can easily report any suspicious illness among their livestock to health officials, who can then quickly follow up with further investigation, if necessary. While this app is still being piloted in several districts of Tanzania and other parts of Africa, it has already been effective in the detection and identification of several small disease outbreaks. I look forward to learning more about Afyadata’s progress.

Polio progress
Going door to door, this hero brings the world closer to ending polio
19 million people who would have otherwise been paralyzed are now walking today thanks to heroes like Shumaila Rehmani.
The world is so close to ending polio.
Since the start of the global eradication effort in 1988, the number of polio cases worldwide has fallen 99.9 percent.
19 million people who would have otherwise been paralyzed are now walking today because of vaccines. And 1.5 million people are alive who would have otherwise died from the disease.
Much of the credit for this progress goes to the thousands of polio workers who have gone door to door vaccinating more than 3 billion children over the last 33 years.
October 24 is World Polio Day and to mark the occasion I’d like to share the story of one of these dedicated polio fighters.
Her name is Shumaila Rehmani.
Shumaila is a polio vaccinator in Pakistan, which is one of the two countries in the world—the other is Afghanistan—where the wild poliovirus is still endemic.
Shumaila’s job is to deliver the polio vaccine to every child under age five in the community she serves. While that probably sounds like a straightforward job, what it takes to get it done is not. Reaching every child requires hard work, meticulous planning, and patience.
During polio immunization drives in Pakistan, Shumaila sets out on foot early in the morning with a cooler filled with vaccines and a detailed plan for all the homes she needs to visit. Then she begins knocking on doors to give the oral polio vaccine drops to every child.
The overwhelming majority of families she visits want their children to be vaccinated. Some parents, however, out of fear or a lack of information, refuse to have their children vaccinated.
But Shumaila doesn’t give up.
She talks with the mothers and fathers, answering all their questions about polio and reassuring them that the vaccine is safe and effective. She also works with community and religious leaders to speak with families about the importance of vaccination.
Progress can be slow. In the community she serves, Shumaila says this year she initially had more than 250 families refuse vaccinations. But today, because of her efforts to work closely with the families, all but four of them have had their children vaccinated. And she continues to talk with those families to encourage them to get vaccinated.
And thanks to the thousands of dedicated health workers like Shumaila and the leadership of Prime Minister of Pakistan Imran Khan, there’s been just one case of wild polio in Pakistan so far this year, compared with 84 in 2020.
While the incredible efforts of Shumaila and other polio fighters have brought us to the brink of a polio-free world, COVID-19 has created new challenges. The pandemic has disrupted polio campaigns and routine immunizations in many parts of the world, causing outbreaks of other forms of polio to crop up in Africa and Asia.
That’s why the global polio program adapted its approach to help contain the spread of COVID-19 while also working to end polio. The Global Polio Eradication Initiative used its workforce and laboratory and disease surveillance network to respond to the pandemic, investigating suspected COVID cases, coordinating response operations, and training health care workers. In Pakistan, the national polio team now operates a toll-free number for anyone who wants to speak with a doctor about COVID, polio, or get any questions answered about routine immunization. They have received more than 17 million calls during the pandemic.
Like other polio workers, Shumaila has used her community relationships to raise awareness of COVID, teach families how to stay safe, and provide handwashing and hygiene lessons. This has made for longer days, but Shumaila says it’s easy to stay motivated. As a mother of three children herself, she is driven by her dream of a day when polio will no longer be a threat to her children or any child in Pakistan.
It’s a day she knows will come soon, she says. Again and again since the start of the global polio eradication effort, one country after the next has eliminated this crippling disease from within their borders. Less than a decade ago, for example, Nigeria accounted for more than half of all wild polio cases worldwide. But last year, Nigeria, along with the 47 countries in the African region, were certified free of the wild poliovirus.
With Afghanistan recently announcing it would conduct a nationwide polio campaign in November—the first in over three years to reach all children in the country—and Pakistan’s continued commitment to eradication, the final two polio endemic countries will hopefully soon follow others on the path to ending wild polio.
“If other countries can be polio free, why can’t Pakistan be?” Shumaila asks.

The sky’s the limit
How David Sengeh is using prosthetic limbs and data science to help Sierra Leone
As chief innovation officer, David is helping his country navigate extraordinary times.
The first time I met David Moinina Sengeh, he was a college senior studying biomedical engineering. The university president asked him to introduce me at a lecture I was giving, and he charmed the crowd by talking about the ways he and I are similar (we both want people to live healthy, fulfilling lives) and how we’re different (our hairstyles). I remember being blown away by his intellect, his ambition, and his sense of humor.
It was clear that David had a bright future ahead of him, but I don’t think anyone could have predicted where he’d end up just a few years later: as Sierra Leone’s first chief innovation officer and youngest ever education minister.
David grew up in Bo, the second largest city in Sierra Leone. His uncle was a surgeon, and David would sometimes get to sit in and observe his procedures. David remembers one time when a woman showed up for her surgery only to be turned away. His uncle explained that the hospital where he worked didn’t have an ultrasound machine, and he wasn’t comfortable performing the procedure blind. Just a few hours later, during a different procedure, the lights went out in the operating room with a patient open on the table.
That’s when he realized what he wanted to do with his life: make sure every health care worker had access to the tools they needed, “I left that day thinking it was great to be a doctor, but I wanted to do biomedical engineering,” says David. So, he went abroad to study—first at a university in Norway and then at Harvard (which is where we met).
Even though he was halfway around the world, David never stopped thinking about how to help people back home—especially the more than 27,000 Sierra Leoneans who became amputees during the country’s civil war in the 1990s. Many of the disabled people he knew growing up chose not to wear prosthetics because they were painful and fit poorly. (I recently wrote about Dr. Mohamed Barrie, another hero from Sierra Leone whose career was also inspired by the same problem.)
So, David decided to spend his doctoral studies designing a more comfortable prosthetic. He ended up creating an innovative new process for fitting prosthetics. It uses an MRI to create a precise measurement of a patient’s remaining limb and a 3D printer to create a socket that fits as close to perfectly as possible.
After finishing his Ph.D. and spending some time in Nairobi studying disease data, David got a phone call that would change his life. Sierra Leone’s new president, Julius Maada Bio, wanted him to come home and serve as his country’s first ever chief innovation officer. He accepted and has been a remarkable advocate for Sierra Leone ever since. David and President Bio even joined me at our foundation’s Goalkeepers event a couple years ago to talk about their work together.
Through his role as CIO, David is working to better integrate technology into every part of Sierra Leone’s government and support the next generation of entrepreneurs. He’s helped develop data visualization tools that local leaders can use to guide decision making. His expertise has been invaluable as Sierra Leone creates new digital tools for its citizens, like a secure electronic health records system. David is doing such a great job that, in 2019, he was asked to take on a second role as the Minister of Basic and Senior Secondary Education.
Just a couple months later, the COVID-19 pandemic started. David has been deeply involved in his country’s response between his two roles.
Sierra Leone didn’t see its first case of COVID-19 until the end of March 2020, but David and his government colleagues started planning as soon as it became clear the virus posed a serious threat. “We had a vision and a strategy that was informed by the numbers from around the world,” he says.
David believes Sierra Leone’s experience during the 2014 Ebola epidemic made them better prepared for COVID-19. He gives credit to the people of Sierra Leone for immediately understanding how important it was to get the virus under control. The population took quarantine restrictions seriously from the beginning. As a result, the country has kept case counts relatively low throughout the pandemic.
Building on David’s work as CIO, Sierra Leone is using a robust data collection system to monitor COVID cases. If you start to feel ill, you can text an automated system to check your symptoms. If you need to quarantine, there’s an app you can use to make sure you receive any supplies needed to stay safe. In turn, local governments are able to use the data collected by these apps to make informed decisions about when to close things down and when to open back up.
The country was also able to reinstate a number of programs created for the Ebola outbreak. For example, in March 2020, David and his colleagues knew that the school closures that were starting to happen around the world would soon become necessary in Sierra Leone. So, they immediately began to rebuild the government’s radio teaching program. Some kids live in parts of the country so rural that radio signals don’t reach them, and the government arranged to have printed materials delivered to them. Kids who lived in bigger cities with internet access were able to take classes online.
Sierra Leone’s ability to implement lessons learned from their last epidemic gives me hope. Although Ebola was devastating for the people of Sierra Leone, the country emerged stronger and better prepared for future public health crises. I’m optimistic the same will be true for the world after COVID-19. “COVID showed us that we have to use technologies that allow us to have an impact,” says David. “This is an opportunity to reset, reimagine, and rethink.”
David Sengeh has achieved so much—and helped Sierra Leone navigate such extraordinary times—that it’s hard to believe he’s only 34 years old. I’m confident that we’ll be hearing about his amazing work for decades to come.
Poop Progress
I need to take a Yee!
Dr. Shannon Yee and his team are developing a new, low-cost toilet to solve the world’s sanitation crisis.
The expression, “I need to take a crap,” originated, at least according to some accounts, with Thomas Crapper, an English plumber and businessman whose name adorned his company’s toilets.
But I hope that this phrase will soon fall out of common usage.
Instead, I look forward to the day when people in search of a restroom say, “I need to take a Yee.”
It would be a great honor for the work Dr. Shannon Yee and his research team have been doing to develop an improved toilet to provide safe sanitation for billions of people around the world.
More than that, if this expression (which Yee fully supports) catches on, it would be a positive sign that our foundation’s efforts to spark a global sanitation revolution have been a success.
That was the dream a decade ago when our foundation challenged the world to create a toilet that doesn’t rely on sewage systems, doesn’t smell, and won’t cost more than a nickel a day to operate. The Reinvent the Toilet Challenge generated hundreds of new innovations in how to process human waste, including toilets and fecal sludge treatment systems that produce electricity, clean water, and fertilizer.
Yee, an associate professor of mechanical engineering at Georgia Institute of Technology, is now leading a group of researchers and private sector partners to take the best of these ideas and package them into a new, low-cost toilet—the Generation 2 Reinvented Toilet (G2RT)—to provide safe, affordable sanitation for the world.
At first glance, Yee may appear to be an unlikely candidate to lead a sanitation revolution. He’s not a sanitation expert. He’s a mechanical engineer who specializes in thermal energy technologies. But those skills are very relevant to how his reinvented toilet operates. It uses heat, energy, and pressure—much like an espresso maker—to process and treat feces.
Still, don’t expect to have a radically different bathroom experience with Yee’s toilet.
How you do your business won’t really change at all.
But what happens to it after will change, dramatically.
In existing toilets, human waste is carried away from our homes by sewers across many miles to treatment centers for processing. While this is a system that has served the world well, it is not sustainable or affordable for the billions of people living with unsafe sanitation. Sewage systems are incredibly expensive, and they waste precious water resources when many people around the planet face severe water shortages.
Instead of relying on a network of pipes and millions of gallons of water to move human waste for treatment, Yee’s toilet processes the poop and pee on site in the toilet itself, which is about the size of a washing machine.
Yee’s toilet has two parts. A frontend, which looks like a typical flush toilet, and a backend, where the waste is processed.
Here’s how it works:
When the toilet is flushed (with a small amount of water), the urine and feces are separated.
The urine and flush water go through a multi-step liquid filtration process that produces clean water. This water is then recirculated to flush the toilet.
And the feces, depending on the model, will take one of two pathways.
In one pathway, the feces get pasteurized, killing off all pathogens and eliminating odors before being pressed into cakes, which are then dried.
In the other pathway, the feces are combusted underwater at 373 degrees in a process known as micro-supercritical water oxidation, producing ash suspended in water.
The water is sent through the filtration process and the ash is dried.
Both the feces cakes and ash then fall into a receptacle that users can dispose of in the trash or compost.
That last sentence may have caught your attention. If there is any major behavior change required with this toilet, it’s emptying the toilet. But that only needs to happen every few days and the waste itself is odorless and pathogen free. It won’t be any more inconvenient than emptying the lint catcher on a clothes dryer.
Currently, Yee’s team is at the end of the development phase, fine-tuning the engineering components of the toilet. Next year, they will be field testing it in South Africa, India, and China. They also plan to have some toilets at demonstration sites in the U.S. and Europe, where Yee expects there will also be demand for a toilet that doesn’t rely on sewers or piped water.
Yee hopes that someday people will think of his toilet as an appliance like a coffee machine or refrigerator. It will be portable and can plug into a wall outlet or run on solar power.
Much more work needs to be done to bring Yee’s toilet to market. Like any mass-produced appliance, Yee’s toilet needs to be durable and simple to maintain and operate, which is why the field testing of the toilet will be critical for identifying any weaknesses in the design.
It also needs to be affordable. The target price is expected to be about $450. While that’s much more affordable than the infrastructure needed to support sewage systems, it may still be too expensive for the world’s poorest families. That’s why it will be critical for donors, governments, and private companies to work together to support the adoption of this new sanitation solution so it can have an impact on the billions of people who need it most.
But I’m optimistic that this toilet has a bright future. And I hope someday soon, you will have the opportunity to “take a Yee” yourself.
Inspiring acts
7 unsung heroes of the pandemic
Incredible people caring for those in need during COVID-19.
When I was a kid, my image of a hero was largely inspired by my dad’s collection of early Superman comics. I read them all. A “hero” was somebody who had supernatural powers like flying, laser vision, or the strength to bend steel.
As humans, of course, we’re all pretty limited in our physical powers. We don’t fly. We can’t see through walls. But what’s unbounded in us is our ability to see injustices and to take them on—often at great risk to ourselves.
My work in global health and development has introduced me to many extraordinary heroes with this kind of superpower. And I’ve had the honor of highlighting many of them on this blog: An epidemiologist who helped eradicate smallpox. A doctor working to end sexual violence in Africa. A researcher working to end hunger with improved crops. Just to name a few.
Why do we need heroes?
Because they represent the best of who we can be. Their efforts to solve the world’s challenges demonstrate our values as a society and they serve as powerful examples of how to make a positive difference in the world. And if enough people hear about their actions, they can inspire others to do something heroic too.
If there’s ever been a time that we need heroes, it’s now. The COVID-19 pandemic has created unprecedented health and economic challenges, especially for the most vulnerable among us. The good news is that many people from all walks of life are doing their part to help them. Health care workers. Scientists. Firefighters. Grocery store workers. Aid workers. Vaccine trial participants. And ordinary citizens caring for their neighbors.
Here are portraits of a few individuals from around the world working to alleviate suffering during this pandemic. I hope their stories inspire you just as much as they have me.
To these heroes and heroes everywhere, thank you for the work you do!

Breakthrough
This virologist’s discovery saved millions of lives and helped launch our foundation
Ruth Bishop’s research uncovered a virus that was killing half a million children a year.
More than 20 years ago, Melinda and I saw a newspaper article about the major causes of childhood death. One disease in particular—rotavirus—caught our attention. The disease, which causes severe diarrhea, was killing half a million children a year…and we had never even heard of it.
In fact, no one had ever heard of it until 1973, when an Australian researcher named Ruth Bishop and her colleagues at The University of Melbourne and Royal Children’s Hospital, Melbourne discovered it.
At the time, Ruth had been searching for the cause behind cases of children with acute gastroenteritis, an infection marked by severe diarrhea and vomiting. It was a common illness around the world, but its impact was greatest in poor countries. When kids in wealthy nations had this condition, doctors gave them a simple rehydration solution. When kids in developing countries had it, they often died from dehydration.
Ruth suspected that some pathogen was responsible for all the illness, but no one had been able to isolate it. Using an electron microscope to examine samples from the hospital’s diarrhea patients, Ruth’s team found what they were looking for. The culprit behind this illness, she learned, was a wheel-shaped virus, earning it the name rotavirus (rota being Latin for “wheel”). Always humble, Ruth attributed her discovery to a “mixture of calculated research and serendipity.”
Rotavirus would become Ruth’s obsession. She went on to research how the virus spread and how to mount a defense against it. And she served as a key leader for the World Health Organization’s efforts to combat rotavirus and other diarrheal diseases. Her breakthrough would eventually pave the way for the development of several rotavirus vaccines and help spur the creation of Gavi, the global vaccine alliance, which has helped to deliver these and other lifesaving vaccines to the world’s poorest countries. Before the first vaccine was available in 2006, more than 500,000 children died of rotavirus every year. By 2016, deaths from the virus had fallen to 128,500.
Still, more work needs to be done to ensure all children can have access to rotavirus vaccines.
Existing rotavirus vaccines are given to infants from six to eight weeks of age, leaving newborns at risk of infection. Thanks to the decades of research led by Ruth, the Murdoch Children’s Research Institute has developed a new vaccine that can be given to babies soon after birth to provide the earliest possible protection from rotavirus.
Hearing about the number of children dying from rotavirus sparked a fire in us many years ago. Thanks to Ruth’s pioneering research and laser focus, her passion for a solution to this overlooked disease became ours.
Melinda and I always had plans to do philanthropy, although much later in our lives. But after we learned about rotavirus, it seemed like there was no time to waste. We started making grants in global health, leading to the creation of our foundation in 2000. Some of our foundation’s first grants went to support the development of an oral rotavirus vaccine. At the time, millions of children in poor countries were not being immunized against deadly diseases like rotavirus. One of our foundation’s largest investments has been to support Gavi’s ongoing efforts to make rotavirus vaccines and other vaccines affordable so all children, no matter how rich or poor, can have access to them.
During our current pandemic, Ruth’s life is a reminder of the importance of scientific research to uncover the unknown pathogens and the power of vaccines to prevent suffering and save lives.
Ruth is now retired, but her legacy continues both as a role model for other researchers who continue to fight against rotavirus and in the millions of children’s lives that have been saved because of her discovery.

Service provider
A gift for mothers and babies
Alain Nteff, a Cameroonian entrepreneur, is using cell phones to save the lives of pregnant women and infants.
For most of us, cell phones are about staying in touch. But in Cameroon, they’re helping to save the lives of pregnant women and infants—thanks to the work of a young entrepreneur named Alain Nteff.
Alain is the founder of GiftedMom, a cell phone app that gives pregnant women and new mothers instant access to medical advice to keep themselves and their babies healthy.
This kind of service would be valuable anywhere, but it’s especially useful in Cameroon, where infant and maternal mortality remains stubbornly high. According to the World Health Organization, Cameroon has the 21st highest under-five mortality rate in the world, and the 17th highest maternal mortality rate. Around 56 babies die each day before they are a month old and 45 stillbirths occur every day, according to Unicef.
Growing up in Cameroon, Alain was aware of his country’s health challenges, but he wasn’t planning on a career in healthcare. He studied computer science in college and had dreams of working for a big tech company. That changed in 2013, when he visited a rural health clinic with a friend, Conrad Tankou, who is a doctor in Cameroon. Walking through the clinic’s wards, Alain came face to face for the first time with babies and young mothers dying.
“The question was, ‘How come in this age with a lot of technology, we still have this problem?’” Alain says.
So, he decided to find an answer.
Alain first explored why Cameroon’s maternal and infant mortality rates were so high. One of the biggest challenges, he learned, was a lack of medical resources. In Cameroon, there were less than 2 doctors per 10,000 people. He also discovered that most women from the poorest households—especially in rural areas—weren’t receiving enough medical care during their pregnancies. Many new mothers would not seek postnatal care for their newborns, leaving them without checkups and vaccinations.
Alain knew that while Cameroon may lack many health resources, many of its people did have a piece of technology that was readily available and might make a difference: cell phones. Working with his friend Conrad, Alain decided to develop a cell phone app to help bridge the gap in care for women and children in Cameroon. He started with a simple SMS system that would remind pregnant women and mothers of their next appointments.
Word spread of the app and one by one the number of subscribers grew from a few dozen to more than 200,000 today. Alain also added other features including medical advice for pregnant women and new mothers, including a due date reminder, regular texts with information about the development of their baby, and basic medical advice about vaccinations and good nutrition.
GiftedMom users also can dial a toll-free number or use a text service to get expert health advice and responses to their questions from a team of medical doctors.
“With technology today, we can democratize access to huge numbers of people. A doctor being on the phone can reach many more users than sitting in the hospital,” Alain says.
While most subscribers to GiftedMom currently use basic cell phones and the app’s SMS features, smartphones continue to grow more popular in Cameroon. Smartphone technology has allowed GiftedMom to add graphics, videos, and other content that will be engaging for mothers. GiftedMom is also developing an online community of mothers who can share stories and learn from one another’s experiences giving birth and raising their children. In addition to a small signup charge, GiftedMom generates revenue to manage the app and create content by charging hospitals a small fee when GiftedMom is used to connect them with a mother.
While the popularity of the app is one measure of success, GiftedMom has already had a positive impact on the country’s health through increased vaccinations and hospital visits. At one hospital in Yaoundé, Cameroon’s capital, the number of women coming for vaccinations jumped from 28,000 per year to more than 40,000 per year. In a rural area of northern Cameroon, GiftedMom helped increase the number of moms going to the hospital by over 60 percent.
GiftedMom’s services are especially important now during COVID-19 when healthcare providers are seeking alternatives to in-person visits, when possible, to decrease the risk of spreading the virus.
Now that the app is having an impact in Cameroon, Alain is looking to release it in other countries in Africa where women are also struggling with a lack of health services. He has a goal of reaching millions of mothers with the app in the years to come.
“The problem of maternal mortality and infant death is not just a mom’s issue—it’s a humanitarian issue,” he says. “And it should not just be women fighting for it. That’s why I’m very comfortable being a man in this space because it’s not just for women. It’s for everyone.”

Inspired by a farmer
These married scientists are leading the way on HIV
The Abdool Karims revolutionized the fight against AIDS. Now they’re helping the world tackle COVID-19 too.
Quarraisha and Salim Abdool Karim are two of the most respected HIV/AIDS researchers in the world. This year, the wife-and-husband team has also helped shape the world’s response to COVID-19. But it was a more humble setting that sparked their careers in epidemiology more than 30 years ago.
They had met in medical school in their native South Africa before moving to New York City for graduate school. In 1988, shortly after they were married, they took a trip to Mexico, where they met up in a tiny village in the Sierra Madre mountains with a friend, a physician who had written a seminal textbook on health care in remote rural settings.
Outside the village’s health clinic, they saw a man pedaling a bicycle that was mounted on a stand and connected to a power cable. It turned out that a local farmer also doubled as the village’s dentist—a pretty good one, apparently—and volunteers would pedal the bike to power his drill.
“We watched how this community took their destiny in their own hands,” says Salim, “and they had the most amazing dental care from this bicycle powering a drill. It imprinted on us how people can really change their own world.”
It was a powerful lesson about the need for scientists to understand and collaborate with the people they’re trying to help. The experience in that village would shape the rest of their careers, especially when they created a research center in South Africa designed to address two of the biggest problems in HIV/AIDS in Africa.
By the 1990s, the disease was devastating the Abdool Karims’ home country—and still is today. One out of every five people in the world with HIV lives in South Africa. The couple saw two issues that were rarely on the agenda of other HIV experts. One was that young women were bearing a disproportionate burden in the epidemic, and that there was no way to control the epidemic if their needs weren’t addressed. The other was that people living with HIV are at a high risk of contracting and dying from tuberculosis—a link that’s now known as HIV-TB coinfection.
“These were very much our problems in Africa that few others were working on,” says Quarraisha, “and if we waited for solutions from elsewhere, it wasn’t going to come. We had to take the lead.”
In 2001, they brought together a group of researchers they felt could make a bigger impact on HIV and named the group CAPRISA (for the Center for the AIDS Program of Research in South Africa). Today CAPRISA runs three clinics where they provide antiretrovirals to people living with HIV and study new approaches to treating and preventing the disease. It is regarded as one of the world’s most influential AIDS research programs.
CAPRISA is probably best known for a landmark study published in 2010 proving for the first time that a microbicide—a gel that a woman could use before and after sex—can offer some protection from the virus. Scientists had been trying to make effective microbicides for nearly two decades, but the Abdool Karims’ formulation—one that used tenofovir, a drug normally given to people who already had HIV—was the first to offer any protection. Although the field has now moved on from microbicides and is focused on a more effective daily pill instead, the concept is still based on CAPRISA’s microbicide findings.
CAPRISA is as admired for the way it works as for its results. Inspired by the farmer-dentist they met in Mexico, Salim and Quarraisha make it a priority to empower the people they’re trying to help. They work closely with community leaders to make sure their research efforts are informed by realities on the ground and embraced by their neighbors. Here’s the story of one remarkable CAPRISA staff member, Gethwana Mahlase, and the way she represents the program in her community of Vulindlela.
Over the next few years, Quarraisha and Salim hope to build on their study of tenofovir as an HIV preventative. Right now, the best option is a pill you have to take every day, a regimen that can be hard to keep up. So CAPRISA is working on a form of the drug that could protect a woman for as long as a year at a time.
They’re also working on a fascinating approach called “broadly neutralizing antibodies,” which dates back several years. In 2012, they discovered that an HIV-positive woman in one of CAPRISA’s studies had a trait that was, as far as they knew, unique. The antibodies made by her immune system could attack not only the strain of HIV that she had, but also—this was the impressive part—80 percent of the other known strains of HIV from around the world. If they could isolate the cells that made these antibodies, reproduce them, and use them to create antibodies for other people, it would be a game changer.
After years of painstaking work with a number of partners, they were able to create the broadly neutralizing antibodies in a lab and test them in monkeys, with very positive results. Now the antibodies are being studied in humans for safety and, eventually, efficacy. If this approach works, you would need to get an injection just twice a year in order to get protection—a dosage that is far more practical than a daily pill. Success would also point the way toward the ultimate goal of an HIV vaccine.
Unfortunately, much of the Abdool Karims’ attention has been elsewhere this year. Drawing on their experiences from HIV and TB, they are helping guide the COVID-19 response in South Africa and around the world. It is a shame that they haven’t been able to focus on HIV/AIDS, but on the other hand, it is a reminder of how fighting old diseases like HIV helps the world prepare for new ones like COVID-19. Investing long-term in programs like CAPRISA—or work on polio or malaria—not only prevents deaths and disability from specific diseases, it also strengthens the overall field of global health. So when a pandemic comes along, we have a network of experts like Quarraisha and Salim ready to pitch in.
What strikes me about this couple is how upbeat they are, even in the face of devastating diseases like the coronavirus and HIV. Their motto at CAPRISA is, “Each day that you come to work, you should be looking for how today is going to be better than yesterday.” That is a lesson we can all take to heart.

Against all odds
This doctor’s life story is almost as remarkable as his work
As a child, Dr. Mohamed Bailor Barrie thought he’d never become a doctor. Now he’s one of Sierra Leone’s health leaders.
Almost everyone who works in global health has an origin story.
Quarraisha and Salim Abdool Karim’s journey to becoming HIV/AIDS researchers started with a trip to Mexico, where they met a local dentist who used a bicycle-powered drill to treat his neighbors. Alain Nteff was inspired to create an app that provides support to pregnant women and new mothers after visiting a rural health clinic. Mine began with an eye-opening trip I took to Africa with Melinda back in 1993.
Dr. Mohamed Bailor Barrie’s story, however, is different from most. Growing up in poverty in northern Sierra Leone, he didn’t have one specific moment where he realized he wanted to work in health. Instead, he saw from a young age how quality health care helps people live better lives.
Mohamed was six years old when he decided to become a doctor. His neighbor was a nurse who treated people out of his home, and Mohamed loved watching him call people’s names one at a time to come in for care. But, for most of his childhood, his dream felt out of reach. There was no medical school in Sierra Leone at the time. To become a doctor, you had to have enough money to study abroad. Mohamed had to sell kerosene and meat by the side of the road just to afford his secondary school fees.
Then Sierra Leone opened its first medical school, and Mohamed earned a scholarship to attend. After he graduated, he turned down job offers from well-paying organizations abroad in order to practice medicine in his home country. “When I was walking back and forth to college, I would see kids suffering,” he says. “After that, I made up my mind to work in Sierra Leone.”
Mohamed chose to focus on a health challenge unique to his country. Sierra Leone endured a brutal civil war from 1991 until 2002. The rebels would often forcibly amputate the limbs of people who they thought supported the government. It’s estimated that around 27,000 Sierra Leoneans were disabled during the war. So, Mohamed helped start an organization called Wellbody Alliance to provide free care to amputee victims.
But it quickly became clear that Wellbody Alliance’s work needed to expand. Mohamed recalls meeting a woman named Khumba while visiting a camp where many amputees lived. Both of the woman’s arms had been removed, but her medical condition had nothing to do with her war wounds: she needed surgery to remove a liver abscess and couldn’t afford the procedure. Mohamed helped arrange to get it taken out and then cared for her while she recovered.
Mohamed and his colleagues decided to open up their clinic to all patients, not just amputees. Wellbody became the primary health care providers for the entire Kono District, providing care for anyone who needed it—from an expectant mother in need of prenatal care to a young person living with tuberculosis and HIV.
Their work took on a new urgency in 2014 when the Ebola virus began spreading in Sierra Leone. Wellbody Alliance teamed up with an amazing organization started by Paul Farmer called Partners in Health to treat the growing number of Ebola patients coming through their doors. “I felt proud that this clinic stayed opened and that we continued to serve patients,” he says. “It’s amazing how heroic our staff was.” Although more than 200 health care workers died from Ebola in Sierra Leone during the outbreak, none of the staff at Wellbody Alliance contracted the virus.
Mohamed also worked with the national government to design a robust contact tracing program. I’m particularly impressed by the system he helped develop to make it easier for people to quarantine. After someone tested positive for Ebola, community health workers would visit the homes of their close contacts. They would encourage them to get tested and talk through the logistics of isolating for the recommended three weeks. If they had any specific concerns—for example, if a family was worried about having enough food to eat—the health workers would contact other local aid groups and arrange for meals to be delivered.
Mohamed’s experience with Ebola helped him prepare for COVID-19. After Sierra Leone recorded its first case in March 2020, he was once again asked to help create the country’s contact tracing program (and to train its participants). Just like with Ebola, each tracer’s approach starts with being sensitive to an individual’s needs. They visit with exposed people in their homes to answer questions, dispel myths, and provide information about how to stay safe.
Although both Ebola and COVID-19 complicated his efforts, Mohamed continues to work towards his goal of improving health in his home country. “I want to see Sierra Leone with a robust health system where people don’t die from diseases that are preventable and where people can have the care that they deserve,” he says. Just last month, he became the new executive director of Partners in Health Sierra Leone. The organization recently broke ground on a new maternal health center in Kono, which Mohamed hopes will become a model for providing comprehensive care to women for the rest of the country.
I can’t wait to see what he and his team will accomplish next. Heroes like Mohamed are the reason we started our foundation more than 20 years ago and why Melinda and I remain committed to its work, even as we enter a new chapter of our lives. In every part of the world, you can find brilliant people doing amazing work to drive progress. It’s an honor to support their efforts to make sure that every person has the opportunity to live a healthy and productive life.

Hope for the future
Meet an epidemiologist fighting to make vaccines work for communities of color
Stephaun Wallace’s work is all about reaching the people who are usually left behind.
If there’s one thing the world has learned about COVID-19 over the last year, it’s this: the pandemic will only end when almost everyone on the planet has been vaccinated against the virus.
Melinda and I have been fighting to expand access to health innovations for the last two decades, so we knew that making the vaccine accessible to all would be a massive challenge. Reaching everyone is going to take a ton of hard work—something that’s become even more clear in recent months. Fortunately, there are a lot of smart, passionate people taking on this problem all over the world. One of those heroes is Dr. Stephaun Wallace, an epidemiologist at the Fred Hutchinson Cancer Research Center. He’s spent the last year helping make COVID-19 vaccines work for everybody.
Stephaun’s road to becoming an epidemiologist is an unusual one. As a kid, he wanted to become a lawyer and help under-resourced people in his community. He moved to Atlanta in his early 20s and created an organization that, among other things, provided assistance to young Black men who were HIV positive. That experience ignited an interest in health inequities and led to a career working to address them.
Today Stephaun wears many hats through his work at Fred Hutch. When he’s not lecturing about global health at the University of Washington, he’s in charge of external relations for both the HIV Vaccine Trials Network and the COVID-19 Prevention Network. (He also found time to speak to my team about systemic racism’s role in the pandemic late last year.)
His work is all about reaching the people who are usually left behind. Growing up Black in Los Angeles, he experienced firsthand how race shapes every part of how society treats you—including the medical system. Stephaun understands why many Black Americans are hesitant to trust doctors and scientists, even though he now counts himself among their ranks. It’s tempting to look to history for an explanation—from the Tuskegee Syphilis Study to Henrietta Lacks—but the COVID-19 pandemic has made it clear that racial health inequities remain a huge problem.
“Acts of racism in the medical establishment are not just historical,” Stephaun says. “People are still very actively experiencing these very same sort of abuses and traumas today.” He points to the case of Dr. Susan Moore, a Black physician who died from COVID-19 last summer after her doctors allegedly dismissed her pain.
One of the reasons why parts of the medical system often fail communities of color is because they’re not designed with them in mind. Stephaun is trying to change that. His work at Fred Hutch is particularly focused on improving the way clinical trials are run. He was working on potential HIV vaccines when the pandemic hit last year and quickly shifted to trials for most of the major COVID-19 vaccine candidates (as well as some treatments).
When you want to test a new vaccine or drug, you have to run rigorous clinical trials to make sure it’s safe and effective for everyone who might take it. Everything from age to race to baseline health can affect how a vaccine works in your body, so it’s important to study how a lot of different people react. Recruiting for a clinical trial can sometimes take longer than running the trial itself—time we couldn’t afford to waste in this pandemic.
The scientists at the COVID-19 Prevention Network knew they had to do a better job of recruiting diverse participants for the multiple COVID-19 vaccine trials they’re running in the Seattle area and globally—especially from Black and brown communities, who are suffering the hardest from the virus and desperately need vaccines that are safe and effective for them.
From the very beginning, Stephaun and his colleagues consulted with expert panels representing these communities to design the trials. They were deliberate about everything from using recruitment tactics tailored specifically for diverse communities to making scheduling more flexible to writing consent forms with accessible, non-scientific language.
The result was a more welcoming experience for all participants. Stephaun reports that the trials saw greater participation from communities of color than he’s used to seeing. He even participated in one of the clinical trials himself, hoping that it will convince more people who look like him that the vaccines are safe.
Stephaun also hopes that the experience of the last year convinces political leaders, the media, and especially his colleagues to reexamine the connection between health and race in the United States. “The pandemic provides the scientific community an opportunity to think differently about how they engage and build relationships with communities of color,” he says. “This offers a reflective opportunity to think about who we are as a culture, as a society, and how we want to move forward.”
Heroes
Walking with a giant
From smallpox to child survival, Bill Foege’s leadership helped keep the global health community together and focused on important goals.
One of my favorite stories about Dr. Bill Foege is the day he arrived in a remote Nigerian village to vaccinate everyone against smallpox. Although most of the villagers were out working in the fields, the chief assured him he could quickly roundup everyone. Bill was doubtful, but soon people began flocking to the vaccination site. By the end of the day Bill and his team had vaccinated several thousand villagers. When Bill asked the chief how he got so many people to show up, the chief replied, “I told everyone to come and see the tallest man in the world.”
At 6 feet 7 inches, Bill is certainly tall in stature. But he stands even taller in reputation. His intelligence, leadership, and humility over the last six decades have proven invaluable in the fight against disease and poverty. In the field of global health, he is a giant.
Bill and I recently had a chance to catch up in Atlanta, where we talked about smallpox, his role as a mentor for Melinda and me, and the stunning progress being made in global health.
Bill is best known for devising a new strategy for eradicating smallpox as an epidemiologist working for the Centers for Disease Control in the 1960s. At the time, the eradication strategy relied on mass vaccination—vaccinating everyone against the disease—but trying to reach the entire population in densely populated urban areas of the developing world proved very difficult. So Bill developed a new approach to stop the virus from spreading by vaccinating a limited number of people—only people who had been exposed to people who were infected. The strategy—which became known as “surveillance and containment”—allowed health workers to respond quickly to outbreaks and saved time and money. This new approach was employed across Africa and India, leading to the official eradication of smallpox in 1980.
(Incidentally, this month marks 40 years since a young man in Somalia named Ali Maow Maalin contracted the world's last case of naturally occurring smallpox. By not passing the disease to any other person, he broke the chain of transmission that had existed for thousands of years.)
The defeat of smallpox did more than bring an end to a disease that killed 300 million people in the 20th century alone. It gave the world the confidence to take on the other eradication efforts, including the global effort to wipe out polio.
In 1984, Bill was instrumental in launching the Task Force for Child Survival, which quadrupled—from 20 percent to almost 80 percent—the proportion of children around the world who receive basic vaccinations. Now known as the Task Force for Global Health, the organization continues to work on a range of health issues affecting the world’s poorest, including river blindness and other neglected tropical diseases. Bill also took on leadership roles as director of the Centers for Disease Control and later director of the Carter Center.
In 1999, Melinda and I were thrilled when Bill joined the foundation as a senior advisor to help us develop a global health strategy. At the time, I was still working full time at Microsoft and I knew very little about global health, but I was eager to learn.
Bill served as our mentor, answering our questions and giving us a crash course in the history of global health. There are few teachers as talented as Bill. As comfortable quoting Voltaire and Democritus as the latest Lancet article or World Health Organization report, Bill is always clear in his thinking about how much the world has accomplished in improving health, as well as how much more we can do to alleviate human suffering.
One of the most valuable contributions Bill made to our learning was giving us a reading list with 81 different books and reports on global health issues. Among them, a book on smallpox (Princes and Peasants – Smallpox in History by Donald R. Hopkins), the history of malaria (Mosquitoes, Malaria & Man: A History of the Hostilities Since 1880 by Gordon Harrison), and a groundbreaking report on the importance of global health investment (Investing in Health: World Development Report 1993).
All these books opened a new world for me, making Bill’s passion for fighting poverty and disease a passion of my own. As l learned more about global health, I discovered that one name appears again and again in accounts about the fights against smallpox and polio to campaigns to wipe out Guinea Worm and improve health care in the developing world. It is Bill’s. While never eager to take the limelight, Bill left his mark on one effort after the next to improve the health of the world’s poorest people.
Looking back at his lifetime of achievements, I view Bill as the glue that held the global health community together, getting it to focus on the right priorities, like raising the immunization coverage, and setting the stage for the progress we’ve seen in global health over the last 20 years.
“It is incredible what has happened. We’ve gone from global health being a total backwater of study. Anyone who wanted to get into it had to discover their own way,” Bill told me. “All that changed and within a few short years it turned out to be one of the most popular subjects in school after school.”
I look forward to seeing what the next generation of public health students will accomplish—by following in this giant’s footsteps.

Game changer
A hero in the fight against the world’s longest-running pandemic
For the last 25 years, Dr. Firdausi Qadri has advocated for an affordable vaccine to save lives from cholera.
While all of us are focused on the COVID-19 pandemic, it’s easy to forget about the world’s longest-running pandemic—cholera. Over the last 200 years the deadly diarrheal disease, which thrives in areas without safe water and sanitation, has killed millions of people. The current cholera pandemic—the world’s seventh—started in 1961, spreading from South Asia to Africa and the Americas. Every year, cholera outbreaks around the globe affect about 4 million people and lead to as many as 130,000 deaths.
An affordable, effective, and safe oral cholera vaccine, however, is proving to be a game changer in the fight against this often-forgotten disease. Thanks in large part to recent cholera vaccination campaigns, the number of cholera cases decreased globally by 60 percent in 2018, according to the World Health Organization. Though 2019 saw an increase in cases, the total number of cholera deaths fell by 36 percent.
This breakthrough has been the life’s work of Dr. Firdausi Qadri, an immunologist and infectious disease researcher in Bangladesh. For the last 25 years, Dr. Qadri has been one of the few people advocating for an affordable vaccine to protect entire communities from cholera epidemics.
While there have been several cholera vaccines since the late 19th century, they were expensive and in short supply. In the early 2000s, the main cholera vaccine available was largely used by travelers from rich countries and was not practical for use in vaccination campaigns of poor communities at risk of the disease.
In 2011, Dr. Qadri and her team at the International Centre for Diarrheal Disease and Research, Bangladesh (icddr,b) led a feasibility study on a newer, more affordable oral cholera vaccine, Shanchol. The study, which was done in partnership with our foundation, showed that the inexpensive vaccine could be an effective tool in stopping the spread of cholera in poor, urban environments, giving people more than 50 percent protection against the disease.
Dr. Qadri’s study—the largest trial of its kind—helped lead to a complete change in thinking about how the world could tackle the challenge of cholera. “You can have very good water, sanitation, education, good homes and people won’t have cholera. But until that happens, you need to stop the misery. You need to control the disease,” Dr. Qadri said. “And the vaccine is a one-stop solution.”
To be sure, access to clean water and sanitation are still critically important for controlling cholera in the long-term. During the 19th century, as cholera spread around the world from its original reservoir in India, outbreaks were eventually brought under control in America and Europe through huge investments in water and sewer systems. And work continues to improve access to clean water and sanitation in low-income countries. But infrastructure improvements can be expensive and take time to build and maintain. Cholera vaccination campaigns provide an important tool to save lives immediately and buy time for communities to pursue longer-term water and sanitation solutions.
In 2013, the WHO helped create an oral cholera vaccine stockpile, to contain and prevent outbreaks. Since then, more than 60 million doses have been shipped worldwide. In addition to Shanchol, a second affordable cholera vaccine, Euvichol, is now available, helping to increase vaccine supplies. Gavi, the Vaccine Alliance, is supporting countries to use the cholera vaccine to target cholera “hotspots”—areas at highest risk—to prevent outbreaks before they happen.
This preventive approach will be even more critical in the years ahead because climate change, urbanization, and population growth create ideal conditions for the spread of cholera. Humanitarian crises are also a breeding ground for the disease. The civil war in Yemen, for example, has led to the largest and fastest-spreading cholera outbreak in modern history, infecting millions and killing more than 3,000 people since 2016.
Still, progress is being made. In Bangladesh, the arrival in 2017 of nearly one million Rohingya refugees from Myanmar into overcrowded camps raised concerns about a cholera epidemic. Working with the government, Dr. Qadri led a vaccination program that has helped prevent an outbreak.
“If this vaccination was not carried out, there would be chaotic conditions,” Dr. Qadri said. “We were able to prevent a major, major epidemic and deaths.”
Successes like this have helped fuel new optimism in the fight against cholera. The Global Task Force on Cholera Control, hosted by the World Health Organization, is a partnership of more than 50 institutions all working together to end cholera. The task force’s strategy aims to reduce cholera deaths by 90 percent by 2030, and eliminate cholera in 20 countries, targeting areas where the disease is endemic and shifting from outbreak response to outbreak prevention.
Thanks to the pioneering work of Dr. Qadri, the world is making progress toward this goal. And maybe someday cholera will be a disease that can truly be forgotten.

Abundant air
Breathing new hope into Africa’s fight against COVID-19
In Africa’s battle against COVID-19, a Kenyan doctor is making sure every breath counts.
As the COVID-19 pandemic spreads across Africa, hospitals across the continent face shortages of essential medical supplies needed to treat the respiratory disease and keep patients alive.
Not just masks and ventilators, but oxygen.
For people living in wealthy countries, medical oxygen is often taken for granted. In many low-income countries, however, oxygen is often in short supply or not available at all. And globally, a lack of oxygen –needed to treat pneumonia, malaria, and other diseases—leads to hundreds of thousands of deaths each year.
Addressing this often overlooked challenge is the life’s work of Bernard Olayo, a Kenyan doctor who founded Hewatele, an innovative organization working to ensure all patients—even in remote areas of the country—have access to oxygen.
Now, he is playing a critical role in Kenya’s preparations to tackle COVID-19 by scaling up oxygen supplies that will be needed to keep the most critically ill patients alive.
While the number of COVID-19 cases in Africa remains low compared to other parts of the world, the continent is bracing for a surge of infections. According to the World Health Organization, up to 190,000 people could die of COVID-19 in Africa if the disease is not controlled. A widespread outbreak would flood many of Africa’s fragile health systems.
A lot of attention has been focused on the lack of ventilators in Africa. Ventilators are the mechanical devices that help patients breathe, pushing air in and out of their lungs, when they can’t on their own. And the shortage of them is a real problem. But the lack of oxygen itself is equally worrying. The coronavirus attacks the respiratory tract, inflaming the lungs and making it difficult for patients to breathe. Oxygen, delivered through a mask or nasal tube, is an essential and effective first line of treatment that’s less invasive than being on a ventilator. Oxygen is also needed to run a ventilator. If COVID-19 patients have access to oxygen as an initial treatment, however, it may prevent many of them from becoming so critically ill that they would require one of the limited number of ventilators to breathe.
What Bernard is hoping to avoid during this pandemic are the painful choices he faced as a young doctor because of a lack of oxygen. After medical school he was posted to a rural hospital, where many of the patients were children battling pneumonia who needed oxygen for treatment. But Bernard soon learned that there was never enough oxygen available. He and the other hospital staff often had to share a single cylinder of oxygen between patients. When there were too many patients and not enough oxygen, he and other doctors would be forced to decide which children would receive oxygen and live, and which would go without it and sometimes die—a choice that broke his heart, he says.
That experience inspired Bernard to investigate the source of Kenya’s oxygen supply shortages. He discovered that one of the biggest challenges is that oxygen is expensive in Africa. In Kenya, oxygen costs about 13 times more than what it does in the United States. The high cost was driven, in part, by a lack of competition. In many countries, including Kenya, there was just a single oxygen supplier for the entire country. And with many health facilities located hundreds of miles away from the oxygen plants, transportation costs drove up prices even higher. The long distances and poor roads also meant that deliveries were unreliable. Hospitals and clinics would regularly run out of oxygen supplies.
In 2014, Bernard founded a public-private partnership to try a new approach that would make access to medical oxygen more affordable and reliable. He named the organization Hewatele (Swahili for “abundant air”). Given the delivery challenges in Kenya, Bernard decided to build oxygen plants at several of the busiest hospitals in the country, where demand is highest and reliable electricity for production is available. The oxygen is then sent out for delivery using a milkman model, with oxygen cylinders regularly dropped off at remote hospitals and clinics and the empty cylinders returned to be refilled. This system ensures that there is always more than enough oxygen available at each facility. Using this new approach, Hewatele has cut the market price for oxygen in Kenya by 50 percent. Now, Bernard is working to expand the number of oxygen plants in Kenya and bring Hewatele’s business model to other parts of Africa.
While the COVID-19 pandemic has brought much needed attention to the oxygen gap in Africa, more needs to be done to ensure that everyone has access to this simple medical intervention. Thanks to Bernard’s efforts, progress is being made. His work has already helped save the lives of thousands of children and adults and will save many more in the future—one breath at a time.

Writing wrongs
This doctor/novelist is tackling malnutrition
The woman behind the promising Grow Great campaign.
Kopano Matlwa Mabaso began her medical education during a terrifying era. The year was 2004, and HIV was devastating whole communities in South Africa, including the township outside Pretoria where she was born. For years, President Thabo Mbeki had denied people access to lifesaving anti-retroviral medicines. When my dad traveled to South Africa with Jimmy Carter to highlight this issue, he watched President Carter nearly come to blows with Mbeki.
To cope with the demands of medical school and the tragedy of what she was seeing all around her, Dr. Matlwa Mabaso started writing her first novel. “It was such a tough time,” she explains. “Writing was debriefing for myself, trying to make sense of all the crazy things I would see.” She published that novel, Coconut, when she was only 21 and still in medical school. It became a bestseller and earned her international acclaim.
But her literary talent did not pull her away from her main goal: helping children grow up healthy so they could contribute to the development of post-apartheid South Africa. After earning her medical degree at the University of Cape Town, she moved to England on a Rhodes Scholarship, studied health-system reform, and earned both her master’s and doctorate in public health at Oxford University. As if these accomplishments were not enough, during these years she wrote two other highly acclaimed novels, had her first child, and started a program to bring mobile ultrasound clinics to the Democratic Republic of Congo.
Today, at age 34, Dr. Matlwa Mabaso lives in Johannesburg and leads the Grow Great campaign, a sophisticated effort to eliminate child stunting from South Africa over the next decade. What is stunting? It’s the physical manifestation of under-nourishment. As the name implies, stunting affects children’s physical development, leaving these children more prone to getting diseases like diabetes and hypertension as adults. Stunting also affects brain development, which means stunted children are less likely to do well in school and less likely to be employed as adults.
Melinda and I have seen many stunted children in our travels. Sometimes we’re talking to a child who looks like one of our kids did at age three only to be told that the child is actually six or seven years old. It’s heartbreaking, and utterly preventable.
In 2016, South Africa conducted a national health survey and learned that a quarter of all children in the country are stunted. “Those results were quite devastating for an upper-middle-income country with the resources we have,” Dr. Matlwa Mabaso says. “Several other countries have less money but much lower rates of stunting than we do.”
Grow Great kicked off in 2018 and hired her as its founding director. She hired a staff of 20 and developed a strategy that draws on successful campaigns in Brazil, Peru, Chile, and other countries that have dramatically reduced stunting in recent years.
Grow Great is scaling up to reach a third of all pregnant women in South Africa—the ones most at risk of having stunted children—with antenatal classes and home visits to empower them to keep their children healthy. There are plenty of challenges Grow Great will have overcome to reach its ambitious goal of zero stunting in the country, but it’s starting with three big advantages.
First, stunting is almost entirely preventable with simple interventions during the mother’s pregnancy (such as making sure she gets nutritious foods) and after birth (breastfeeding, a healthy diet, and other steps for mother and child). Second, the South African government has great health policies that are aligned with the best data from global health institutions like the World Health Organization. Third, the country has nearly 70,000 community health workers, many of whom were originally hired and trained as a response to the HIV crisis. With training and support from Grow Great and its partners, these health workers are now providing not just education but also immunizations and other health services to pregnant and new mothers.
Grow Great has also launched a mass-media campaign—including social media, billboards, and taxi signs—to support its work on the ground. One big focus of the campaign has been promoting breastfeeding. Some new mothers prefer formula because they see it as a signal that they’re not poor. Others resist breastfeeding because of the lasting stigma from the early years of the HIV epidemic, when mothers were told that they could pass the virus to their children through their breastmilk. “There remains a lot of mixed messaging and stigma in communities around HIV and breastfeeding that we still need to overcome,” says Dr. Matlwa Mabaso.
As a natural outgrowth of her public health training, she put in place rigorous measurement systems from the beginning of the campaign, including efforts to listen to the mothers Grow Great serves and make adjustments accordingly. “We’ve already learned a lot from listening,” she says. “For example, in a lot of cultures here in South Africa, traditional practice is that babies can’t leave home for their first three months. So in these communities, postnatal classes outside the home for new moms just don’t work. We had to recreate the model.”
Grow Great is now one year into its implementation. Preliminary data are promising. For example, the data show that moms are recognizing the importance of early stimulation and nurturing care while the baby is in the womb. The data also show that participating in antenatal classes is helping new moms cope with the demands of pregnancy and the prospect of a new baby. In the next few years Grow Great will evaluate the impact of these efforts, assessing whether stunting is actually decreasing and, if so, by how much.
In her rare moments of quiet, Dr. Matlwa Mabaso will continue to use her writing talents to make sense of both the empowering and challenging days of working on one of South Africa’s most pressing public health problems. She and her husband, an engineer, have their hands full with demanding work and raising two children. But she has no intention of letting her writing muscles atrophy. “I don’t know if it will be another book, but I’m doodling and scribbling all the time,” she says.

Like father, like daughter
Bangladesh’s dynamic duo battle global health inequity
A father-daughter team is working to reduce child mortality in Bangladesh.
As a little girl growing up in Bangladesh, Senjuti Saha remembers how dinner conversations in her family often focused on bacteria, viruses, and infectious diseases.
Those topics might strike many people as a little gross at mealtime, but in the Saha family that’s what happened when her father, Dr. Samir Saha, brought his work home. A professor of microbiology, Samir used family dinner to practice his scientific lectures or share what he was learning about Bangladesh’s health challenges. (I wish I could have had a seat at the table—I love learning about diseases!)
Those conversations had a big impression on Senjuti, who went on to become a microbiologist herself. Dr. Senjuti Saha now works with her father at the Child Health Research Foundation (CHRF), an organization he helped found to reduce child mortality in Bangladesh and other countries.
Together, the father–daughter team are a dynamic duo of global health. They are working to close the gap in healthcare delivery between low-income countries, where child mortality is high, and wealthier countries, by using data, state-of-the-art diagnostics, and vaccines to battle infectious diseases. Their research is not only being used in Bangladesh, but by other countries in South Asia facing similar health challenges.
Thanks to the work of the CHRF, along with strong support for childhood immunization and health care by the government, Bangladesh continues to push down its under-5 mortality rate and improve overall healthcare delivery. Vaccine coverage in Bangladesh, a country of 170 million people, has now reached 98 percent.
Samir, who also heads the department of microbiology at the Dhaka Shishu Hospital in Dhaka, played an instrumental role in helping Bangladesh introduce vaccines for meningitis and pneumonia, two major childhood killers. While those vaccines were available in the U.S. and other rich countries, they were not in low-income countries like Bangladesh. Working diligently to document the burden of these diseases, Samir provided the data and evidence to convince public health policymakers to support the rollout of both vaccines, which have already prevented thousands of deaths.
Senjuti focuses on finding simpler ways to diagnose mysterious illnesses in poor countries that affect newborns and children. In 2017, when there was an unexplained spike in meningitis cases among children in Bangladesh, Senjuti was able to unravel the mystery by analyzing the genetic material of the children. (The meningitis cases, she discovered, were caused by an outbreak of Chikungunya fever, a virus spready by mosquitos.) But in order to get to the bottom of the mystery, she had to fly the samples to the U.S. for analysis. She’s since set up a low-cost diagnostic tool in Bangladesh to help the country quickly address future outbreaks of meningitis and other deadly diseases.
The information that the Sahas are gathering from their research is critical for Bangladesh, which lacks many of the resources needed to diagnose and treat illnesses. The data CHRF gathers is helping to inform government policy decisions for the most effective ways to combat diseases. It is also being used to design new vaccines.
Even as conditions improve in Bangladesh, however, the country has a long way to go. Speaking at this year’s Goalkeepers event, Senjuti shared a powerful story that captured the huge health challenges that remain in Bangladesh. At Dhaka Shishu Hospital, Bangladesh’s largest pediatric facility, more than 6,000 children are refused admission every year because its 665 beds are always full, and many of the beds are occupied by people suffering from preventable diseases. Many of the children turned away need immediate care.
If Bangladesh can do more to prevent diseases, however, it can free up resources to focus more on the illnesses that can’t be prevented. Thanks to the work of Samir and Senjuti, Bangladesh is moving toward a future of fewer infectious diseases and more available hospital beds.

Gone viral
Meet the virus hunters
These scientists are doing amazing work all over the world to stop infectious diseases like Ebola.
It’s hard for me to overstate how brave people who willingly put themselves on the frontlines of outbreaks are—especially when you’re up against an enemy we haven’t seen before. Without any information about how a disease jumps from person to person, it’s difficult to protect yourself. Your only option is to put on a biohazard suit and trust that it will keep you safe.
If you’re a health worker in a situation like that, you’re often faced with patients you can’t help. We can’t treat a disease until we know what it is, after all. That’s where virus hunters come in.
Virus hunters are given a near-impossible task: find out where a mystery pathogen came from, how it’s transmitted, and how to stop it. Although they’re scientists and researchers by training, they also have to be detectives. A good virus hunter must look for clues and follow leads until they catch the bad guy. Think True Detective, but with microscopic pathogens instead of serial killers.
Virus hunters are doing amazing work all over the world to stop infectious diseases (including those caused by bacteria and other pathogens—the name is a bit misleading!). I want to introduce you to two examples that I find particularly inspiring: the doctor who tracked down one of the most infamous diseases in human history, and a team of rock star scientists that deploys to outbreak zones on a moment’s notice.
The real-life Sherlock Holmes who helped discover Ebola
When I picture the quintessential virus hunter, one name comes to mind: Dr. Peter Piot. I’ve spent a lot of time with Peter over the years, and I never get tired of hearing him talk about the case that made him famous.
Peter was just 27 years old when the Belgian lab where he was working received a blood sample infected with a then-unknown disease. In 1976, most people thought infectious diseases were a thing of the past—but health officials were starting to worry about a new sickness in Zaire (today called the Democratic Republic of the Congo) that caused people to bleed until they died. Peter and a team of researchers around the world worked together to identify the mystery virus, which we now know as Ebola.
But identifying a virus on a microscope is only the first of many steps to stopping an outbreak. So, with no real idea of what he was up against, Peter headed to Zaire to hunt for patient zero. He and his colleagues drove from village to village in a Land Rover, collecting information about who was sick and where they had been before symptoms appeared.
Eventually, Peter spoke to a group of nuns who noticed that people seemed to get sick after they attended the funeral of someone who died from the disease. That tip led to a key revelation: Zairean mourners washed their dead. After they touched the bodies—which were often covered in blood—the mourners would eventually rub their eyes or put their fingers in their mouths. A week later, they’d get sick.
That understanding helped Peter and the other virus hunters understand that Ebola spreads through contact with a sick person’s body fluids. Once we knew how the disease was transmitted, it was a lot easier to limit its spread and stop the outbreak before it reached a critical level.
Peter’s experience with Ebola was just the beginning of a long career fighting infectious disease. He was one of the first microbiologists to study AIDS, and in 1995, he became the founding executive director of UNAIDS. During his 13-year tenure, he coordinated the global response to HIV/AIDS through the discovery of the first treatments for the disease and the peak of the pandemic. After a brief stint at the Imperial College London and as a fellow with our foundation, he became the director of the London School of Hygiene and Tropical Medicine where he still teaches today.
The Avengers of virus hunters
Peter isn’t the only virus hunter in residence at the London School of Hygiene and Tropical Medicine, though. In partnership with Public Health England, the school also hosts the UK Public Health Rapid Support Team (or RST)—a heroic supergroup of scientists who deploy to outbreak zones to help local governments stop infectious diseases.
In just a little more than two years since it was created, the RST has already assisted in controlling 11 outbreaks in seven countries. The team has deployed to scenarios ranging from a diphtheria outbreak at a Rohingya refugee camp in Bangladesh to a plague flareup (yes, that plague) in Madagascar.
Here’s how the RST works: as soon it becomes clear that an outbreak is underway, the local government (or, in rare cases, the WHO) requests their help. Not every team member is needed for every outbreak—sometimes you need an epidemiologist and a data scientist but not a microbiologist—so the first step is to identify who needs to go. The chosen team then has 48 hours to get their visas squared away, pack up any special equipment, and get to the airport for their flight to the outbreak zone.
Once on the ground, they either build a mobile laboratory or set up their equipment to supplement what’s already there. The team then gets to work supporting local health officials. The tools they have at their disposal are a lot more high-tech than the ones Peter used back in 1976 (including gene sequencing, which they use to decode the genetic makeup of viruses). This technology helps the RST work with local experts to target the origin of the outbreak and limit its spread.
A typical deployment lasts six weeks. If the outbreak is still ongoing at the end of that period, the current team heads home to London, and a new team takes their place. For example, the RST has been on the ground in the Democratic Republic of the Congo since the beginning of the latest Ebola epidemic there. When they’re not in the field, the team spends their days researching how to better respond to outbreaks and helping countries improve their capacity to control disease emergencies.
I’m really glad that the United Kingdom invested in a team like this, the Rapid Support Team’s work is an important part of a global coalition that makes all of us safer. We don’t know when—or where—the next major disease outbreak will emerge. It could arrive next month, next decade, or next century. And in a world where you can fly nearly anywhere in less than a day, there are no guarantees the next epidemic will remain confined to the other side of the world from you. The ability to respond to a disease is crucial for protecting the world from the next pandemic, and I hope more countries follow the U.K.’s lead.

No kidding
Can goats empower women?
A group of Indian health workers is helping poor women gain financial independence by raising goats.
Can goats empower women?
In one of the poorest areas of India, they already are.
This is thanks to a new team of health workers who are training rural women how to gain financial independence by raising healthier goats.
The health workers are goat nurses known as “pashu sakhis,” which means “friends of the animals” in Hindi. Pashu sakhis are all poor women themselves who are given basic training in how to vaccinate, deworm, and provide other preventive care to goats in their community.
So, how does this help empower women?
In India’s poorest rural families, goat rearing is an important source of income. Goats can be sold easily because they are always in demand as a source of food. In fact, goats are nicknamed “ATMs” because of they are a convenient source of cash.
Unlike more valuable operations on farms in India—crops or cattle, for example—goats are managed almost exclusively by women. They bring them out for grazing, take care of them when they’re ill, and sell them at the market.
And here’s the most critical point—the money women earn from their goats stays in their hands. With more control of their finances, women not only improve their status within the homes, but they also have greater ability to make decisions and have greater power over their own lives. Study after study shows that when women have cash, they will spend it on things that improve the quality of life for their family. That means more money for buying food to improve nutrition, schooling for children, visiting a doctor, or even building a toilet.
India has more than 135 million goats—one-sixth of the world’s goat population. And more than 70 percent of poor, rural families raise them. So, there is huge potential for goats to help boost women’s empowerment. But that potential has not been fully realized. Because of a lack of access to veterinary services in India, mortality rates for goats are as high as 40 percent. And ill or low-weight goats fetch lower prices in the marketplace.
That’s why the pashu sakhis are so important. They are filling a gap in these veterinary services to help improve the health of the goats. Through a program called Project Mesha run by the Aga Khan Foundation and supported by our foundation, more than 200 women are being trained to be pashu sakhis in four communities in the Indian state of Bihar. Bihar is one of the poorest states in India and has one of the country’s largest populations of goats. Working through local women’s groups, the program aims to increase incomes for 50,000 of India’s poorest women by 30 percent.
A key part of the project is to ensure that the pashu sakhis are empowered themselves. They charge small fees for their veterinary services, which provide them with a source of income and a financial incentive to promote goat care in their communities. In Bihar, local culture allows husbands to place tight restrictions on their wives’ mobility and decision-making power. But as pashu sakhis earn more income from their goat services, they say they are also gaining more respect and independence from their husbands.
While this project is still small, it has potential for huge impact for poor women in India. The Aga Khan Foundation is working with the government of Bihar to expand the program in other districts in the state.
At our foundation, we want to see more women’s empowerment projects like this one. That’s why last year we launched a new strategy focused on gender equality, which focuses on removing the barriers to equality that women and girls face so they too may live a healthy, happy, and economically productive future.
Unless we all push for greater equality, women will not have the opportunity to reach their full potential, nor will the communities where they live. Thanks to the incredible work of the pashu sakhis, thousands of women in India will now have an opportunity to break out of poverty and exercise greater power over their lives.
TB Determined
Good news in the fight to stop one of the world’s oldest diseases
We’ve finally moved into the next phase of the fight against tuberculosis.
When you work in global health, you see a lot of sickness and tragedy. You never get used to it, but after years of visiting hospitals and clinics, I thought I knew generally what to expect.
Nothing could prepare me, though, for the drug resistant tuberculosis ward I visited in Durban, South Africa in 2009. Every bed was filled, and the waiting list for admission was more than 80 names long. The worst part was the floor that was just for children, including several infants. One baby had XDR-TB, the deadliest and most difficult to treat form of drug-resistant TB. It was truly awful to see.
Soon, however, TB hospitals in South Africa may look very different. Recent scientific breakthroughs mean that many of the wards that used to be full of patients may one day be filled with empty beds instead. That’s a testament to the incredible efforts of TB researchers around the world. One of those amazing scientists is Dr. Andreas Diacon, who founded an organization called TASK.
Dr. Diacon started his career as a TB specialist in Switzerland, where he rarely treated more than five patients at once. TB kills more people than any other infectious disease, but few of them are in level 4 countries like Switzerland. Because he was able to spend so much time with each patient, he got to know the ins and outs of the disease better than most. He eventually ended up in Cape Town, overseeing a clinical trial for the first new TB drug in decades.
TB research stalled in the late 20th century, because existing drugs were seen as sufficient, and there was little financial incentive to create new ones. In 2005, Dr. Diacon created TASK to help accelerate the development pipeline for novel TB treatments. The organization started with a staff of five and has grown to 180 employees. They’ve overseen trials of multiple drugs that are now being used to cure patients, including some with drug-resistant TB.
Drug resistance develops when a TB patient takes an insufficient amount of drugs to cure the disease. If a patient doesn’t finish a full course of medication, the bacteria that causes TB can mutate and become resistant to the most common forms of treatment. That mutated bacteria can then spread to other people. About one out of every 20 patients that Dr. Diacon sees has some form of drug resistance.
Even XDR-TB is curable, but not everyone responds to the treatment, and it is pretty brutal. The most common method requires daily injections for up to two years. Because those injections can only be done by a professional, patients who don’t live near a clinic often have to remain hospitalized even after they’re no longer contagious. The drugs can cause a whole range of terrible side effects, including nausea, fatigue, and even hearing loss.
Luckily, there appears to be a better way to treat XDR-TB. Researchers have identified a new three-drug cocktail that requires only six months of treatment. Instead of painful injections, patients take a fixed number of pills (the exact number depends on your weight and age) once a day.
The new course has fewer negative side effects than the injectable one, and there’s no risk of causing deafness. It’s also outpatient based, so people don’t have to stay in the hospital while receiving treatment. Plus, it’s cheaper than other treatments.
Some of these new drugs are already saving lives in South Africa. The country has the highest rate of drug-resistant TB infections per capita in the world, in large part because of the ongoing HIV epidemic (three out of every five TB patients in South Africa are also HIV-positive). With the old, injectable treatment, only 60 percent of those patients were still alive after 50 weeks of treatment. Today, with the new three-drug cocktail, 87 percent survive. That’s a remarkable increase.
Tuberculosis has haunted humanity for millennia—it’s even been found in Egyptian mummies. For most of that time, we had no clue how to stop it. Scientists finally found a cure in the mid-1900s, but it was imperfect, and innovation stalled for decades. Thanks to brilliant scientists in South Africa and around the world—including the team at TASK—we’ve finally moved into the next phase of the fight against tuberculosis.
Mass protection
All Hail the Condom King
With creativity and fun, Mechai Viravaidya has helped save millions of lives by promoting easier access to contraception.
I’ve never met anyone who knows how to have as much fun with condoms (in public, anyway) as Mechai Viravaidya.
The social activist from Thailand has fashioned the contraceptives into colorful hats, dresses, shirts, suits and other sartorial creations. (Mechai once gave my dad a baseball hat made from hundreds of condoms. He wore the cap at our foundation’s annual meeting, earning big laughs from the staff.) He’s started school contests to see who could inflate a condom into the biggest balloon, persuaded Buddhist monks to bless them with holy water, and convinced police to hand them out on the street (a program he dubbed “cops and rubbers”).

All this fun had a serious goal—to destigmatize contraceptives in a culture where talking about safe sex and family planning was taboo. Mechai’s efforts have been so successful that he is affectionately known as “Mr. Condom,” or “The Condom King,” in Thailand.
Mechai never sought this condom crown. Born in Thailand to a Scottish mother and Thai father—both of whom were doctors—Mechai trained as an economist and started his career at Thailand’s economic planning agency. It was there that Mechai discovered that his country was experiencing alarming population growth. At the time, the average Thai family had seven children and the annual population growth rate was over 3 percent. Most women didn’t have—or even know about—basic birth control.
Worried about Thailand’s future, Mechai decided to launch an organization called the Population and Community Development Association (PDA) in 1974 to promote family planning. From the start, he took an unorthodox approach to promoting safe sex. At the time, Thailand had few doctors, so PDA trained nurses and midwives to educate couples about family planning strategies. In a country where most people were uneasy discussing sex, Mechai pushed the conversation out into the open. He made contraceptives readily available from the smallest roadside stand to the biggest stores and taught people that there was no reason to be shy about talking about sexual health. He won over his audiences with humor, using condoms as batons in school relay races and hosting vasectomy festivals where men were rewarded with a free hot dog for undergoing the procedure. Thanks to these and other efforts, Thailand’s annual population growth fell from 3.2 percent to less than 1 percent today.
Mechai’s work with PDA helped prepare Thailand for its biggest health challenge of the 1980s and 1990s: HIV/AIDS. When the AIDS epidemic came to Thailand, Mechai and PDA responded with prevention programs targeting those at greatest risk, including sex workers and their clients. PDA launched roving HIV testing vans and established AIDS education theme nights in the country’s red-light districts.
Later appointed head of Thailand’s national HIV program, Mechai continued to challenge taboos in Thai culture by persuading taxi drivers to hand out condoms to their passengers and launch attention-grabbing safe sex campaigns, including condom ads painted on to the side of elephants. Believing that everyone needed to be involved in the health challenge facing Thailand, he partnered with the military to run public service announcements about HIV on the radio. Thailand became one of the first countries in the world to achieve a decline in HIV infections. New cases of HIV decreased by 90 percent from 1991 to 2003.
The world can continue to learn from Mechai’s efforts to expand access to contraceptives. Far too many people become infected with HIV each year. Too often, the people facing the greatest risk—including young women, sex workers, men who have sex with men and people who use drugs—do not have access to the contraceptives they need to protect themselves.
Better access to contraceptives is also critical for family planning. When couples have access to contraceptives—including ones that women control, unlike condoms—they are more likely to have smaller families, women are freer to work outside the home, and fewer women die from unsafe abortions or pregnancy-related complications. Communities benefit too because parents can devote more resources to their children’s health and education—setting them up for more productive futures.
Mechai’s contributions to Thailand have gone well beyond his success promoting family planning and HIV prevention. He was elected three times to serve in Thailand’s senate. To raise money for PDA, he launched a chain of restaurants named Condoms and Cabbages (because condoms should be as plentiful as cabbages in Thailand, he says). The restaurant’s motto is “our food won’t make you pregnant.” He also started a school and fought rural poverty through a village development program to support community entrepreneurship and empowerment.
Mechai’s extraordinary life and work in global health and development has helped improve the lives of millions of people in Thailand. And the Thai people have thanked him with an honor that is perhaps the greatest measure of his impact. When people in Thailand want a condom, they don’t call it a condom. Instead, they refer to it by the name of the man who taught them the importance of using one—they ask for a “Mechai.”
Welcome center
What I learned from a teacher of refugees
She told me her students “are innately hopeful.”
When I was a student, I was lucky to have some inspiring teachers—including a wonderful librarian when I was in the fourth grade and a chemistry teacher in high school—who challenged me and brought out my best. They helped make me the person I am today.
I recently met a remarkable teacher who is doing the same thing for kids who face obstacles I never could have imagined when I was in school. Her name is Mandy Manning and she teaches English and math in Spokane, Washington, to immigrant and refugee teenagers who have just arrived in the United States. They come from all over the world: Syria, Guatemala, Afghanistan, Myanmar, Sudan, Mexico, Tanzania, even Chuuk State. They show up at school speaking little or no English. Some have fallen far behind in other subjects after months or years of living in refugee camps. Mandy is the first teacher they encounter in this country.
In recognition of her work, Mandy was named Washington state’s 2018 Teacher of the Year. She also had the big honor of being named National Teacher of the Year for her efforts to “help her students process trauma, celebrate their home countries and culture, and learn about their new community.” Like other recent Washington teachers of the year (see here, here, here, and here), she was nice enough to visit my office so I could learn more about her and her students.
Mandy teaches at Ferris High School’s Newcomer Center, which was created in 1997 specifically to help immigrant and refugee students make the transition to living in the U.S. I’ve been going to Spokane for years to visit relatives there, so I know a bit about the city, but I was surprised to learn how diverse the student population is. Mandy told me 77 different languages are spoken in the district. It’s not unusual for her to have a class with 12 students who speak eight different languages.
“A lot of the kids have come through trauma to get to the United States,” Mandy told me. “They've faced war, extreme poverty, religious and political persecution, the loss of family members. And it’s not automatically the land of milk and honey when you get here. They have days where they’re struggling with culture shock or post-traumatic stress. Now it’s gotten a little bit worse because people feel more empowered to say really hateful things.”
Even so, Mandy says her students are “innately hopeful, because they came out alive.” “The kids are so excited to be in school,” she said. “It’s a moment in their day where they know what is expected.” They’re generally at the Newcomer Center for one semester before transitioning to Ferris or one of Spokane’s other high schools. They spend five periods a day with Mandy, learning English and math, and one period with another teacher working on basic computer skills like how to use software and navigate a website. They interact as much as possible with their peers at Ferris High, going to pep rallies and sporting events and staffing the student store. It’s a great way to make friends, practice their English, and get to know their new community.
Mandy shared some of her students’ unforgettable stories. She told me about a 14-year-old Sudanese girl who arrived at the Newcomer Center in 2012 after spending much of her life in a refugee camp in Kenya. The girl had a fourth-grade education and spoke very little English when she arrived in Spokane. But through a ton of her own hard work and support from her teachers, she graduated from high school in four years. Today she’s enrolled at a university here in Washington state, where she’s studying to be an elementary school teacher.
I hadn’t met many National Teachers of the Year before, so I asked Mandy what that’s been like. She’s not in the classroom this year—instead she’s visiting schools and talking with educators across the country. She compared it to the time she served in the Peace Corps in Armenia. “It’s mostly about cultural exchange,” she said. “I bring back what I learn, and they hopefully have learned a little from me.”
In addition to listening and learning, Mandy is using her platform to champion ideas about education that she has developed in her 19-year career. She’s a big advocate for making sure kids see how their classes are relevant to their lives; she said when that happens—when you’re really engaged by your studies— “you can be a time traveler, seeing yourself in the future going to a university.” She is also calling attention to the disparities between high- and low-income schools. And she argues persuasively that teachers need more of a voice in setting education policies. (She wrote an excellent post here on TGN on that point.)
Hearing Mandy talk about her students reminded me of one of the biggest strengths of America’s public schools: They are intended to help every child succeed. The fact that some places fall short of that ideal should not obscure the successes that are happening in Spokane and other cities across the country. And behind every one of those successes are super-talented, hard-working teachers like Mandy Manning.
Heroes
Recovering Rwanda
Dr. Agnes Binagwaho helped turn Rwanda into a global health success story.
In 1994, Rwanda was torn apart by a brutal genocide that killed nearly one million people. Its economy and health system were in ruins. Many of the country’s doctors and health workers had been killed or fled. Fewer than one in four children were vaccinated. A cholera epidemic swept through refugee camps. It had the world’s highest child mortality rate and the shortest life expectancy. Rwanda’s future appeared bleak.
Today, Rwanda is a stunning global health success story—one I often cite when I’m asked about examples of health and development progress. More than 97 percent of infants are vaccinated. Rates of child mortality, maternal mortality, and deaths from tuberculosis, AIDS, and malaria have all plummeted. Its health system has become a model for other nations to follow.
Many people were involved in making this dramatic turnaround possible—from government leaders to health workers to the people of Rwanda themselves. Even today, Rwanda hasn’t let up; the country is determined to build on its gains. But the story of Dr. Agnes Binagwaho is a great illustration of what it took to make this transformation possible.
As a physician, leader of Rwanda’s HIV program, and later minister of health until 2016, Dr. Binagwaho has spent the last two decades playing a hands-on role in helping to rebuild the country’s health care system.
Born in Rwanda but raised in Europe, she moved back to Rwanda after the genocide to help with the reconstruction. At the time, Rwanda’s health system had so few resources that when Dr. Binagwaho would return from trips abroad she would fill her suitcases with medical supplies to help care for her patients.
The transformation of Rwanda’s health system has its roots in a very simple, but powerful idea promoted by the government of Rwanda. It’s the belief that health is a human right for all—no matter their income, ethnic group, or where they call home.
“The lesson of the post-genocide period for Rwanda—and for countries around the world hoping for recovery from social upheaval of many kinds—is that a nation’s most precious resource is its people,” Dr. Binagwaho wrote in a Lancet article documenting Rwanda’s recovery while she was minister of health.
To reach the poorest families, Rwanda trained thousands of community health workers who travel from home to home providing care. The government built rural health posts to expand access to medicines and health services. They also launched a nationwide health insurance program. At the heart of the government health care program is establishing trust between the government and the communities they serve. The health workers, for instance, were selected by the villages they served, so the people could decide who would care for them.
While much more work needs to be done to continue to strengthen health care, Rwanda’s progress has been remarkable. That the country’s health system has managed to achieve so much progress on a limited budget compared to other poor countries is often called a “miracle.”
Dr. Binagwaho is quick to correct that misconception and steer credit to the country’s people. “It’s everything except a miracle. It’s the hard work of thousands of health professionals,” she says. “Everything that Rwanda has done is one way or another replicable.”
Sharing what Rwanda has learned about health care is the goal of Dr. Binagwaho’s new career in academia. After leaving the ministry of health in 2016, she was appointed vice-chancellor of the University of Global Health Equity, a university dedicated to educating health care professionals about how to improve health care among the world’s poorest people.
Founded in 2015 by the nonprofit health care organization, Partners in Health, and funded in part by our foundation, the university seeks to radically change the way health care is delivered around the world. The new approach focuses on training a new generation of health care professionals to provide more equitable health services and meeting the world’s most pressing health challenges—including containing diseases like Ebola and designing and running better health care systems.
Currently based in Kigali, the university is building a new campus in the rural community of Butaro in northern Rwanda. The remote setting will allow students to experience first-hand how Rwanda’s effective system of health care delivery is improving the lives of the poor. I look forward to the impact the university’s graduates will have on the future of global health as they help share the lessons of Rwanda’s success with the rest of the world.
The last mile
This doctor wants to make sure no patient is out of reach
Dr. Raj Panjabi’s quest to reach people in remote places.
It is amazing how many lifesaving tools you can carry on your back.
I was meeting with Dr. Raj Panjabi, and he was showing me one of the backpacks created by Last Mile Health, the nonprofit he co-founded in Liberia. Raj reached into the bag and took out a vial of medicine to treat pneumonia. Next he pulled out rapid test kits for malaria and HIV. Then, rehydration salts for children with diarrhea. A measuring tape to screen kids for malnutrition. A thermometer to check for fevers. A blood pressure cuff. And so on. It was like watching a magician pull rabbits out of a hat.
The backpack is a key part of Last Mile Health’s effort to deliver basic health care to people who live beyond the reach of the health system. Raj was born in Liberia and fled the civil war there with his family when he was 9. When he returned as a medical student years later, he was shocked to learn that there were only 51 doctors for a country of 4 million people. So he and his co-founders set out to recruit, train, and equip a cadre of community health workers who would provide a range of 30 basic services in remote areas of Liberia.
Thanks to Last Mile Health, more than 500 trained workers now serve 280,000 people in two of Liberia’s most far-flung counties. “These are community members,” Raj told me, “who may have a middle-school to a high-school education and can be trained and equipped to provide high-impact medical care just within a matter of weeks.” (Our foundation helps fund some of their work.)
Other countries use community health workers too—I’ve written before about Ethiopia’s success with them and will be posting soon about Rwanda’s—but Last Mile Health is putting some clever twists on the idea. For example, they’re on the cutting edge when it comes to using digital tools. Their staff use smartphones to collect data about their work with patients, which helps identify health trends and improve the program. They’re also developing a training platform where you could watch video lessons on, say, how to vaccinate children, or hear a podcast on how to distribute bednets, and then take a quiz to test your understanding.
Ultimately, there’s no getting around the need for a primary health care system with well-stocked clinics and staff. Community health workers are a good complement to a functional primary health care system, and a step in the right direction for places that don’t yet have one (like Liberia). As Raj says, no one should die simply because they live too far from a doctor. It’s great to see him and his colleagues trying to make that idea a reality. We need more passionate innovators like them.
Heroes
“We can change hate by love.”
Dr. Denis Mukwege and his hospital staff have cared for more than 50,000 survivors of sexual violence.
Dr. Denis Mukwege is founder of Panzi Hospital in the Democratic Republic of Congo, where he and his staff have cared for more than 50,000 survivors of sexual violence. They include women who have been raped in front of their families and girls brutally assaulted by combatants during the country’s two decades of civil war. Some of his patients are infants—less than one-year-old—who have been raped.
For someone who has witnessed so much cruelty and suffering, Dr. Mukwege could be forgiven for not having a very hopeful view of our world. But when I met him in New York last year, I was struck not only by his warmth and gentleness, but also his incredible optimism.
“What is keeping me going is really the strength of women. I discovered how women are strong, how women can rebuild, and give hope for our humanity,” he told me. “They have taught me a lot about how we can make our world better, by not only thinking about yourself but to think about other people.”
As a boy growing up in eastern Zaire (now the Democratic Republic of Congo), Dr. Mukwege was drawn to a life of service to others. He would accompany his father, a pastor, as he went from home to home to pray for the sick in their community. While he admired his father’s faith, he wanted to use the power of medicine to help heal them. At age 8, he decided he would become a doctor.
He went to medical school in France where he specialized in pediatrics. As he learned about how many women were dying giving childbirth, especially in his own country, he switched to obstetrics.
When he returned to Africa, he opened a center to provide maternity care in the city of Bukavu in eastern Congo. It was the first clinic of its kind in the entire region. But the first patient he saw didn’t come because she was pregnant. She had been raped and shot. In the months that followed, dozens more rape survivors showed up at his hospital. By year’s end, Dr. Mukwege had treated hundreds of survivors and their numbers kept growing. He soon learned that rape was being used by soldiers to intimidate and displace entire communities, causing the women and their families to flee.
“When rape is used as a weapon of war, the impact is not only to destroy women physically, it’s also to destroy their minds . . . to destroy their humanity,” he said.
At first, Dr. Mukwege focused on treating the women’s physical wounds. But he soon realized that it was not enough. Most of the women had been so traumatized that they could not go back home and restart their lives. So, he designed a more comprehensive approach to care that goes beyond physical healing and focuses on psychological support and socioeconomic assistance. He also started a legal program to pursue justice for the survivors of sexual violence.
Looking back over the thousands of patients he’s seen over the years, Dr. Mukwege says one case stands out for him. It’s the first patient he treated—more than two decades ago. She underwent six surgeries and, at first, was unable to walk. She thought her life was ruined, he recalled.
But she was inspired to help others who had experienced what she had. She enrolled in school and dedicated her life to taking care of other victims of sexual violence. Today, she is one of the longest serving employees at Panzi Hospital, where she helps patients put the pieces of their lives back together. Thanks to her efforts and the work by the rest of Dr. Mukwege’s staff at Panzi Hospital, thousands of women have been able to rebuild their lives—some even going on to become nurses, doctors, and lawyers.
“The goal is to transform their pain into power,” Dr. Mukwege said. “We can change hate by love.”
Heroes
Strength in numbers
The story of this amazing woman living with HIV in Mozambique fuels my optimism about our world.
Last year, at an event in New York, I learned about an impressive woman whose story I want to share with you. Her name is Cacilda Fumo, she lives in Mozambique, and every year she helps save hundreds of lives—by reminding them they are not alone.
Mozambique has one of the highest HIV infection rates in the world. More than 1.6 million people—10 percent of the adult population—are living with HIV.
Cacilda was diagnosed with HIV in 2002. “When I first learned about it, I thought I would die,” she recalls. “I used to wake up early morning and check if I am alive or not.”
But then she started meeting other people living with HIV, and as their numbers grew so did her strength and her belief she would live. Cacilda was one of the first in Maputo to be open about her status. She started wearing a t-shirt emblazoned with a logo that reads: “HIV POSITIVE.”
At times, people rejected her because of her status. Many more in her community, however, admired her for her courage, helping her create an even larger circle of friends and supporters. They met every week, praying together, cooking together, and sharing their stories. Eventually, the group had about one hundred people, many of them receiving life-saving anti-retroviral treatment. Cacilda emerged as their leader.
About the same time, Mozambique’s Ministry of Health was struggling to improve the delivery of anti-retroviral treatment. While the program was successful in putting thousands of patients on treatment for the first time, medical staff were overburdened with caseloads. People on HIV treatment often walked miles to reach their clinic and waited in long lines to get care. Every year, about 30 percent of HIV patients dropped off their life-saving treatment.
Working with Doctors Without Borders, the government of Mozambique decided to try a new approach to simplify care to help keep more people on treatment. They started organizing small peer support groups for people on HIV treatment. The idea was simple. Make treatment easier by putting more control into the hands of the patients. A representative from each patient group could pick up all the drugs for the group each month, saving the rest of the group the hassle of going to the clinic. Members of the groups, known as Community antiretroviral therapy (ART) Groups or CAGs, would also support one another to ensure they were all staying on their treatment.
When the program reached Maputo, Cacilda was ready to join. She helped organize dozens of support groups from her network. Then she went one step further. She kept track of the groups, checking whether members were attending their meetings and taking their treatment. If someone fell off treatment, she took upon herself to locate them and find out what was wrong.
“We help people feel strong knowing they are not alone,” she says.
Some patients who stop treatment are addicted to alcohol and forget to take their treatment, she says. Some don’t understand how the treatment works and the stop taking their medication as soon as they feel better. Others get busy with their jobs and drift away.
Whatever the reason, Cacilda warns them of the dangers of stopping treatment and encourages them to restart. Her efforts to bring back residents of Maputo to treatment has become nearly full-time work. Most days residents of Maputo see Cacilda traveling on foot—which is remarkable because due to a childhood injury she uses crutches—through the dirty alleyways and crowded markets in search of people who have stopped treatment. She doesn’t give up until she finds them.
Cacilda’s persistence pays off—in lives saved. Cacilda estimates that she tracks down about 500 people every year and encourages them to resume their treatment.
That’s a remarkable achievement—one that proves how much difference one life can make in the world.
Outside the box
A humanist approach to teaching kids
I recently met a school superintendent who has some creative ideas about how to help students.
Education is one of the most challenging areas our foundation works on. There will never be a medicine that guarantees every child has access to a world-class education or a vaccine to prevent kids from dropping out. Each district has unique needs, and a good idea that works in one school might be difficult to scale across the entire system.
Melinda and I have evolved our thinking about education over the years, but one thing we remain committed to is innovation. I try to meet regularly with teachers and administrators in the field who have creative ideas about how to make school systems work for every child.
I recently had an insightful conversation with one of these big thinkers: Jorge Aguilar, the superintendent of the Sacramento City United School District. Although this is only his first year running his school district in Northern California, he’s already making a real difference in the lives of his students.
Jorge’s approach as an educator is shaped by his personal story. His parents were migrant farm workers from Mexico, and he split his childhood between a small town in California and his family’s hometown. When his senior year of high school came around, his parents didn’t know enough about the U.S. system to help him apply to college. He didn’t even know how community colleges differed from universities until a representative from the University of California visited his school.
Today, Jorge uses data to make sure kids like him don’t slip through the cracks. Twenty percent of the students in the Sacramento school district are still learning the English language, and approximately 70 percent are classified as low-income—two groups that are particularly at risk for falling behind academically. Jorge helped develop an early-warning system that looks at attendance, behavior, and academic records to detect kids who are more likely to drop out. His district also uses national college acceptance data to create recommendations for seniors about where they should apply.
“Data can keep you very human as long as you remind yourself that every numerator, every denominator is the face of a child,” he told me. “There’s just so many ways in which we can use data for this idea of making our work more human and taking a humanist approach.”
Jorge is also a big believer in what he calls an “opt-out philosophy” (it has nothing to do with opting out of tests). If a student excels at a particular subject, she gets automatically enrolled in college prep and other classes such as Advanced Placement. If she’s falling behind, the school signs her up for additional winter or summer classes. In both cases, parents must sign a form saying they don’t want their child to participate if they want to opt out.
He first implemented this approach in his previous job with the Fresno Unified school system. Jorge knew from the data that more Fresno students could benefit from extra instruction than were currently enrolled in summer school. Before the program, the entire district would see only four or five students sign up every year. After switching to an opt-out system, an impressive 18,000 students attended summer classes. He is now implementing a similar program in Sacramento.
I hope that eventually no child will need remedial instruction to succeed in the classroom. Until that day comes, I’m glad more students are getting the help they need. It’s too early to tell if Jorge’s approach is working in Sacramento, but I’m excited that he’s willing to try something new. I can’t wait to see the results.
Heroes
On the doorstep of victory
Millions of courageous vaccinators have brought the world closer than ever before to the end of polio.
The world is closer than ever before to wiping out polio.
Last year, the world saw the fewest number of polio cases—just 21, according to the latest figures.
That’s incredible, especially when you consider that just 30 years ago, there were 350,000 cases of polio per year worldwide.
The heroes who have made this progress possible are the millions of vaccinators who have gone door to door to immunize more than 2.5 billion children. Thanks to their work 16 million people who would have been paralyzed are walking today.
But the job is not over. The few polio cases left can be found in three countries: Afghanistan, Pakistan, and Nigeria. Many of the vaccinators in these countries continue to work in difficult and dangerous conditions to protect children from this paralyzing disease.
They deserve our thanks and support as we work toward the day when no child is at risk of polio.
Heroes
No masks or capes, but these heroes are saving the world
They may be too humble to call themselves heroes, but there’s no better way to describe them.
In many ways, being a philanthropist is easy. Although our foundation funds a lot of efforts to help improve the world, I sacrifice little compared to the people doing the hard work that makes progress possible. I’m not a vaccinator in Afghanistan combatting polio, an agricultural extension officer in India helping farmers grow more food, or a teacher standing in front of a class each morning to do one of the toughest jobs I know—preparing the next generation to succeed in college and life.
These and millions of other people like them are making a difference in our world. And while they may be too humble call themselves heroes, I can think of no better word to describe them.
I wanted to call attention to some heroes among us. They are just a few of the many people using their talents to fight poverty, hunger, and disease and provide opportunities for the next generation. To all of them, wherever they are, let me say thank you. The world is a better place because of what you do.
Here are the stories of five of these heroes. Their lives inspire me. I hope they’ll inspire you too.
1.
Dr. Segenet Kelemu
As a young girl growing up in a poor farming village in rural Ethiopia, Segenet Kelemu once witnessed a swarm of locusts wipe out the crops in her village. She vowed then to use the power of science to find ways to help farmers grow more food and earn more income.
She decided to study agriculture, becoming the first woman from her region to get a college degree, went on to graduate school in the U.S. and working in an international research institute in South America. After working abroad for 25 years as a plant pathologist, she returned to Africa in 2007 to lead a new generation of scientists dedicated to helping the world’s smallholder farmers grow more food and lift themselves out of poverty. She is currently director general of the International Center for Insect Physiology and Ecology in Nairobi.
2.
Dr. Mathew Varghese
The elimination of polio from India in 2011 is one of the world’s greatest public health achievements. While there are no new polio cases in the country, thousands of the disease’s survivors still live with the impacts of the crippling disease. Dr. Mathew Varghese, an orthopedic surgeon at St. Stephens Hospital in Delhi, runs India’s only polio ward, where he provides reconstructive surgery for polio patients to give them greater mobility. He looks forward to the day when he has no more patients to serve.
3.
Dr. Adaora Okoli
In 2014, Ada Okoli, a Nigerian doctor, made international headlines when she became infected with Ebola while caring for her patients in a Lagos hospital. I met Ada a few years ago, and heard her harrowing story of survival. She has now dedicated her medical career to the research, treatment, and prevention of future epidemics. Her courage and her optimism are inspiring.
4.
Anna Rosling Rönnlund
Anna Rosling, the co-founder of Gapminder, is dedicated to using art and science to help us make sense of a complicated world. One of my favorite examples of her work is Dollar Street, where she uses photos and big data to create an engaging portrait of how people live around the world. Thanks to her efforts we can see ourselves and our world more clearly.
5.
Camille Jones
Camille Jones is the 2017 Washington State Teacher of the Year. Raised on a farm in rural Quincy, Washington, she returned to her hometown in 2010 to be a teacher. Using hands-on learning approaches, she leads a schoolwide effort to inspire students to explore the possibilities that science, technology, engineering, arts, and math can offer. Thanks to her work, she’s helping more students in our state dream big.
World AIDS Day
The fight against AIDS is filled with heroes. Learn how you can be one too.
Thanks to many heroes, the world has made amazing progress against HIV/AIDS.
On December 1st, the global community will observe World AIDS Day. This year I would like to mark it by highlighting the work of two heroes who are making a difference in the fight against this deadly disease.
Chief Jonathan Eshiloni Mumena is chief of the Kaonde people, who live along Zambia’s border with the Democratic Republic of Congo. Risking his position as his people’s leader, Chief Mumena challenged long-held traditions to encourage Kaonde men to embrace voluntary medical male circumcision as a strategy to prevent HIV transmission. (Male circumcision can reduce a man’s risk of acquiring or transmitting HIV by up to 60 percent.) I had the privilege of meeting Chief Mumena in 2012. His story is an inspiring tale of courageous leadership and deep compassion for his people.
Guided by her belief that health care is a basic human right, Dr. Krisana Kraisintu, a pharmacist from Thailand, has worked tirelessly to make medicines affordable to even the poorest in the world. Her development of generic versions of the lifesaving HIV drugs dramatically reduced treatment costs, saving and improving countless lives. She has also dedicated her pharmaceutical skills to reduce treatment costs for malaria and other diseases.
Of course, Chief Mumena and Dr. Kraisintu are just two of the countless individuals—doctors, policymakers, researchers, activists, and political leaders—whose contributions have helped turn the tide against the disease. Today, 19.5 million people receive lifesaving antiretroviral therapy, giving them the opportunity to live full, productive lives. Improved access to treatment has also meant that millions of babies are now born HIV-free.
Much of this progress has been made possible by the world’s enormous investments in efforts to defeat the epidemic, including the Global Fund to Fight AIDS, Tuberculosis and Malaria, and the U.S. HIV/AIDS program known as PEPFAR, President’s Emergency Plan for AIDS Relief.
Still, many challenges lie ahead in the fight against the AIDS epidemic.
Funding for HIV control has been flat and there’s talk about cuts as the world turns to other priorities. Cuts in funding for HIV/AIDS would lead to sharp increases in deaths and new infections, reversing the gains that have been made the last decade. That’s why it’s more important than ever for the world to reaffirm its commitment to this fight. We need more AIDS heroes—from health care workers and advocates to global leaders. Together, we can bring an end to this public health threat.
If you want to be a hero this World AIDS Day, support the (RED) Shopathon. Our foundation is matching every dollar raised—up to $15 million—to fight HIV/AIDS in Africa.